
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
Why Stress-Related Tension Is a Biological, Not Just Mental, Issue
Stress-related tension is not a mental problem with physical symptoms. It is a biological event — measurable, structural, and traceable to a nervous system that never received the all-clear signal.
When the brain perceives a threat, the amygdala signals the hypothalamus to flood the cardiovascular and neuromuscular systems with epinephrine. Heart rate climbs. Arterial pressure rises. Skeletal muscles activate, braced for immediate physical action. That response is built to be short. Under chronic stress, it does not turn off.
Sustained autonomic arousal produces measurable hyperactivity in the muscles — particularly the trapezius — even at rest. Elevated resting muscle electrical activity correlates directly with high anxiety indices. The nervous system keeps telling the muscles to stay ready. The muscles comply. Relaxation becomes physiologically incomplete.
The damage continues at the tissue level. Sustained sympathetic activation causes vasoconstriction in peripheral muscle groups. Oxygen delivery drops. Metabolic waste accumulates, triggering localized pain and trigger points. The HPA-axis — the brain-body stress communication pathway — dysregulates under chronic load, driving elevated cortisol that directly sustains muscle fiber contraction. The clinical result is myofascial pain syndrome: physical, structural, and traceable to a nervous system stuck in threat mode.
The alarm keeps firing not because the danger is real — but because the off-switch is broken.
Over time, asymmetric muscular pull from stress-locked fibers creates mechanical joint restrictions. Chronic muscular tension alters spinal biomechanics. Severe cognitive work demands correlate strongly with clinical neck and shoulder pain. The body stops repairing soft tissue micro-tears because the repair window never opens.
This is stress as a physical load — one the spine and nervous system are carrying right now, whether the mind acknowledges it or not. Treating it requires understanding what is actually locked, where, and why. Not a generic protocol. Not a breathing exercise.
Last Updated: June 22, 2026
- • Your Nervous System Doesn't Know the Meeting Is Over
- • What Chronic Stress Actually Does to Your Spine and Muscles
- • The Brain-Body Feedback Loop Nobody Tells You About
- • What a Systems-Biology Assessment Actually Looks At
-
• Frequently Asked Questions
- • Why does mental stress cause physical muscle pain in my neck and shoulders?
- • What is the biological link between chronic stress and physical misalignment?
- • How does the nervous system lock skeletal muscles into a state of chronic spasm?
- • Can targeted chiropractic care break the biological feedback loop of stress-related tension?
- • Why don't standard stretching and relaxation techniques resolve chronic somatic tension?
- • The Alarm Doesn't Turn Off on Its Own
Your Nervous System Doesn't Know the Meeting Is Over

The meeting ends. The calendar clears. Your mind knows it's over.
Your nervous system doesn't.
The amygdala doesn't read your schedule. It reads threat signals — cortisol levels, muscle activation patterns, cardiovascular load. It responds to what the body is carrying, not what the mind decides.
When that load has been stacking for months, the off-switch doesn't flip back when the workday ends.
The alarm keeps firing. Not because danger is present — because the sensor is stuck.
That distinction is everything. It's why stress-related tension doesn't resolve on its own — not with time off, not with mindfulness apps, not with a long weekend.
Why the Stress Response Wasn't Built for a 40-Hour Work Week
The fight-or-flight response was built for a sprint. The amygdala fires, the hypothalamus responds, epinephrine floods the cardiovascular and neuromuscular systems, arterial pressure climbs, and skeletal muscles load for immediate physical action.
That sequence is brilliant for escaping a physical threat. Run it on repeat across a 40-hour work week and it becomes physiologically catastrophic.
Repeated epinephrine surges damage blood vessels and drive up muscle resting tone. The muscles never fully return to baseline.
The body's natural repair window — the low-threat state where soft tissue micro-tears actually heal — gets crowded out by the next activation cycle. Severe cognitive work demands correlate strongly with clinical neck and shoulder pain because the tissue never gets the recovery window it needs. The CDC documents this directly: occupational stress isn't a mental health issue. It's a driver of musculoskeletal disorders.
Patients describe the same pattern without prompting: the tension in their neck and shoulders never fully disappears — not on weekends, not on vacation, not after two weeks away.
That's not psychological sensitivity. Research published by NIH confirms it's a measurable biological cascade with physical consequences that accumulate structurally. For anyone dealing with nervous system stress recovery in Morton, IL, the starting point isn't relaxation — it's understanding that the nervous system was never designed to sustain the volume of perceived threat that modern work life delivers.
The Cookie-Cutter Response to Stress Tension Gets It Wrong
So what does the standard response look like? Breathe. Reframe. Relax.
Those aren't wrong recommendations. They're just aimed at the wrong layer of the system.
Running the same adjustment protocol on every stress-tension patient — same sequence, same depth, same frequency regardless of what the nervous system is actually doing — doesn't resolve the structural load. It moves pieces without addressing the driver.
A cookie-cutter response to structural failure isn't a care plan. It's a template. When the driver is an autonomic system locked in chronic activation, repeating the same intervention is the clinical definition of not paying attention.
What's required is chiropractic care that starts with assessing what's actually locked — which joints, which muscle groups, which autonomic patterns — and builds from there.
Not from a protocol. From the patient's clinical picture.
That's the difference between treating the alarm and turning off the sensor.
| Stress Signal | Nervous System Branch Activated | Immediate Physical Effect | Chronic Physical Consequence |
|---|---|---|---|
| Perceived workplace threat (deadline, conflict, pressure) | Sympathetic nervous system (fight-or-flight) | Epinephrine floods cardiovascular and neuromuscular systems; heart rate climbs; skeletal muscles activate | Blood vessels sustain repeated damage; muscle resting tone rises and never fully resets |
| Unrelenting cognitive demand across a standard work week | Sympathetic nervous system (sustained activation) | HPA-axis engages; cortisol levels elevate; muscle fiber contraction is maintained | Myofascial pain syndrome develops; soft tissue repair window closes before micro-tears can heal |
| Persistent low-grade occupational stress (email overload, task switching, performance pressure) | Sympathetic nervous system (chronic arousal) | Trapezius and surrounding muscles maintain elevated electrical activity even at rest | Clinical neck and shoulder pain emerges as structural — not just symptomatic — consequence of cognitive load |
| Absence of physical resolution signal (no 'all-clear' from the body) | Parasympathetic nervous system (suppressed — cannot override) | Autonomic off-switch fails to engage; vasoconstriction persists in peripheral muscle groups | Metabolic waste accumulates in muscle tissue; trigger points form; spinal biomechanics shift under asymmetric muscular pull |
| Mental attempt to de-stress (vacation, journaling, meditation) | Parasympathetic nervous system (partial engagement at best) | Cortisol drops temporarily; perceived relaxation occurs at the cognitive level | Structural muscle lock and joint restriction remain — sensor is still stuck; alarm keeps firing |
What Chronic Stress Actually Does to Your Spine and Muscles
You feel it in your neck mid-meeting. You roll your shoulders between calls. You call it stress.
But what's happening in the body isn't a feeling. It's a structural event — and it's been building long before you noticed it.
Here's what that shoulder roll isn't fixing.
Sustained psychological stress triggers a measurable physiological cascade through the autonomic nervous system. The muscles don't just feel tight. They're electrically hyperactive — held in elevated resting tone that the nervous system is actively maintaining, not passively allowing.
That distinction changes everything.
This isn't tension waiting on a good night's sleep. It's tension the body is generating deliberately — because the autonomic system hasn't received the signal that the threat is gone.
Muscle Lock: How the Body Physically Encodes Stress
The trapezius muscles sit at the intersection of the cervical spine, the shoulder girdle, and the upper thoracic column. Under chronic stress, they become ground zero.
Not because they're weak. Because they're the first place the autonomic system cashes its checks.
NIH research on autonomic stress documents it directly: autonomic nervous system arousal prevents complete skeletal muscle relaxation, and elevated resting muscle electrical activity correlates with high subjective anxiety indices.
In plain terms: the more stressed the nervous system, the higher the baseline electrical activity in the muscles — even when the person is sitting still, doing nothing, thinking about nothing stressful.
The body doesn't need an active stressor to stay locked. It just needs the off-switch to stay broken.
And it doesn't stay in the muscle.
Asymmetric muscular pull from stress-locked fibers creates mechanical joint restrictions. One side contracts harder than the other. The joint loses its normal range. Chronic muscular tension alters spinal biomechanics over time — not as a metaphor, but as a measurable structural outcome.
This is how chronic stress becomes a spinal problem without a single traumatic event.
Microcirculation Failure and Trigger Point Formation
Here's what most people miss.
The damage isn't just in the muscle fiber. It's in the blood supply feeding it.
Sustained sympathetic activation causes vasoconstriction in peripheral muscle groups. Blood vessels narrow. Oxygen delivery drops.
Published research on microcirculation confirms that decreased oxygen delivery accelerates metabolic waste buildup in the tissue — and that buildup creates the localized, self-sustaining pain loops known as trigger points.
The body isn't producing that pain arbitrarily. It's producing it because the tissue is starved.
Trigger points aren't just sore spots.
They're knots of ischemic tissue — muscle fibers starved of oxygen and saturated with metabolic waste, locked in contraction because the conditions that would allow release never arrive.
That's the biology behind why the same spot in your upper back hurts every single week. It's not a mystery. It's a supply problem the body can't solve on its own.
The Postural Collapse That Comes After the Tension
So what happens when the tension never fully breaks?
When stress-locked muscles pull asymmetrically on the spinal column for weeks or months, the joints begin to adapt. Mobility decreases. The spine shifts its load distribution. Misalignment follows — not from a single incident, but from the cumulative weight of an autonomic system that never fully powered down.
The spine is compensating for a nervous system that won't stand down. That compensation has a structural cost.
At Touch of Wellness Chiropractic, this is exactly what Dr. Karen Hannah's assessment is built to find.
Which joints have lost mobility. Which muscle groups are maintaining that loss. Which autonomic patterns are driving the cycle.
A standard protocol doesn't assess those layers — it skips them entirely. An individualized assessment starts there. That's the difference between massage therapy that moves pieces and chiropractic care that matches the structural reality the body is actually living in.
| Biological Mechanism | Tissue or System Affected | Structural Outcome | How It Presents Clinically |
|---|---|---|---|
| Autonomic nervous system arousal triggers EMG hyperactivity | Trapezius muscles and cervical muscle groups | Elevated resting muscle tone — muscles held in sustained contraction even at rest | Persistent neck and shoulder tightness that doesn't release after rest or sleep |
| Elevated anxiety indices correlate with elevated resting electrical activity | Skeletal muscle fiber — full-body muscular system | Chronically elevated baseline tone with no spontaneous reset | Muscles feel "always on" — tension present even during low-demand activities |
| Sustained sympathetic activation causes peripheral vasoconstriction | Muscle tissue microcirculation — peripheral blood supply | Reduced oxygen delivery and accelerated metabolic waste accumulation in muscle fibers | Localized trigger points — dense, ischemic knots producing predictable, recurring pain |
| Asymmetric muscular pull from stress-locked fibers | Spinal joints — cervical, thoracic, and lumbar segments | Mechanical joint restrictions and loss of normal spinal mobility | Reduced range of motion, joint stiffness, and pain with movement in specific spinal segments |
| Chronic muscular tension alters spinal load distribution over time | Spinal biomechanics — vertebral alignment and posture | Cumulative structural misalignment as the spine adapts to asymmetric muscular forces | Postural deviation, uneven shoulder height, and chronic mid-back or low-back pain with no single injury event |
The Brain-Body Feedback Loop Nobody Tells You About
The fight-or-flight response doesn't fire and reset.
It leaves a physical residue — in the tissues, the joints, and the nervous system pathways that ran the whole cascade.
That residue becomes the loop's input signal.
The brain reads the body's physical state — elevated muscle tone, restricted spinal mobility, compressed joint range — and interprets it as evidence the threat hasn't passed. So it keeps the alarm running. Not because the stressor is still present. Because the body never structurally signaled that it was gone.
This is the car alarm blaring in an empty parking lot.
The sensor isn't responding to danger anymore. It's responding to its own stuck state. And no amount of deep breathing resets a sensor — because the sensor isn't a thought. It's a physical structure carrying a physical load.
How the HPA Axis Translates Thought Into Tissue Damage
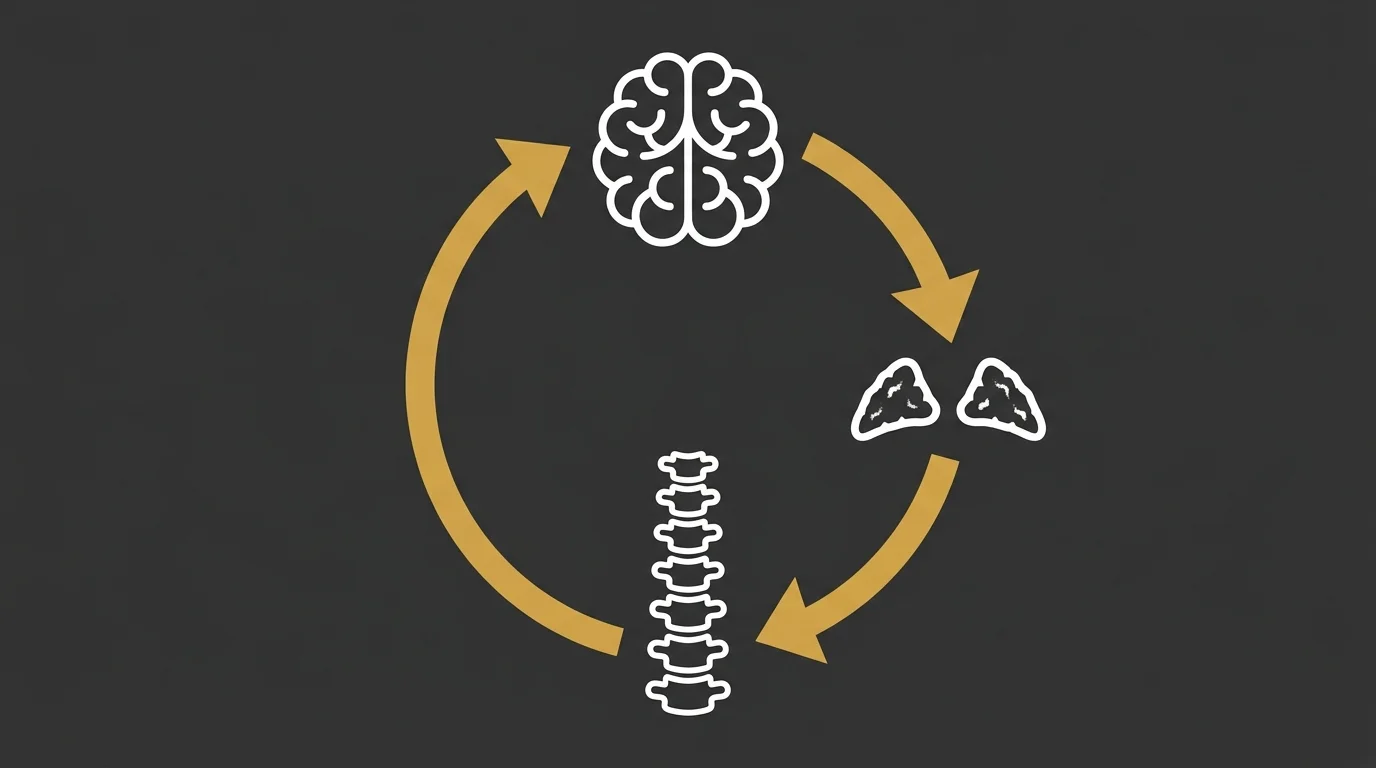
The HPA axis — the hypothalamic-pituitary-adrenal pathway — is the brain's direct line to the body's stress chemistry.
The amygdala reads a threat signal and activates the hypothalamus. The hypothalamus triggers the pituitary. The pituitary signals the adrenal glands to release cortisol. That cascade was designed to be temporary. A short burst, a resolved threat, a return to baseline.
Under chronic stress, it isn't temporary.
NIH findings on HPA dysregulation confirm that ongoing HPA-axis dysfunction directly correlates with somatic pain severity — and that chronically high cortisol levels contribute directly to sustained muscle fiber contraction. The muscles aren't tight because you're anxious right now. They're tight because the cortisol signal never stopped telling them to contract.
That sustained contraction produces myofascial pain syndrome.
It looks like muscular soreness. It isn't. It's the downstream result of a brain-to-tissue chemical signal the nervous system keeps transmitting — week after week, whether the patient is under active stress or not. The tissue damage isn't originating in the muscle. It's originating in the HPA pathway that's been dysregulated for months. And that's exactly what the chronic stress and physical misalignment connection reveals — the source is upstream, and the muscle is just where you feel it.
Why 'Just Relax' Doesn't Release the Physical Lock
Here's what makes this feedback loop so clinically stubborn.
The physical state of the body becomes its own threat signal. The amygdala reads muscle tension, restricted joint mobility, and elevated cardiovascular tone — and responds by keeping the sympathetic nervous system activated. Relaxation techniques don't interrupt that loop. They don't change the physical input the amygdala is reading.
Epinephrine floods the system, spikes arterial pressure, and primes skeletal muscles for immediate action. That's what it was built to do — once.
But repeated surges of the same signal increase muscle resting tone and damage blood vessels over time. By the time someone describes their shoulders as "always tight," that elevated baseline has been locked in long enough that the nervous system treats it as normal. It's not tension anymore. It's the new floor.
"Just relax" doesn't work because relaxation is a cognitive instruction.
The lock isn't cognitive. The joints have restricted. The muscle fibers are maintaining elevated electrical activity. The cortisol signal is still running. What turns the alarm off isn't a mindset shift — it's an individualized assessment that identifies what's physically locked, and a care plan built to address those specific layers. Not a template built for someone else's nervous system.
| Intervention Type | What It Addresses | What It Misses | Why the Tension Returns |
|---|---|---|---|
| Deep breathing / meditation | Conscious cognitive state in the moment | Elevated muscle resting tone, restricted spinal joints, ongoing cortisol signal | The physical input the amygdala is reading never changes — so the sympathetic response restarts |
| Stretching and mobility work | Temporary range of motion at the surface level | Underlying joint restrictions and the autonomic patterns maintaining them | Mobility returns briefly, then the stress-locked musculature pulls the joint back into restriction |
| Massage therapy alone | Soft tissue tension and local circulation in the session | Spinal joint mobility loss and the neurological feedback loop driving the tension | Muscles re-tighten as the nervous system reasserts the same elevated baseline it was never structurally reset from |
| Cookie-cutter chiropractic protocol | Spinal segments according to a fixed sequence — not the patient's actual locked pattern | Which specific joints are restricted, which muscle groups are maintaining that restriction, and which autonomic pathways are driving it | The protocol addresses what it always addresses — not what this nervous system is actually doing |
| Individualized chiropractic assessment and care plan | The specific joints, muscle groups, and autonomic patterns identified through clinical evaluation of this patient | Nothing — because the care plan is built from the clinical picture, not a template | Tension resolves because the structural input driving the feedback loop is directly addressed — the sensor gets turned off, not just ignored |
What a Systems-Biology Assessment Actually Looks At
Most assessments start with the symptom. Where does it hurt? How long? What makes it worse?
That's a reasonable place to start. It's the wrong place to stop.
A systems-biology assessment starts somewhere else entirely: the nervous system's current operating state.
The pain isn't the problem. The pain is the output — structural evidence left behind by a system that's been running in threat mode long enough to reshape joints, muscle fibers, spinal biomechanics, and the autonomic patterns holding all of it together.
That's a different clinical question.
Not "where does it hurt" — but "what is the nervous system doing, and what has it done to the surrounding structure?"
That answer is what builds the care plan. Not a protocol handed down from the last patient.
Reading the Nervous System Before Touching the Spine
Dr. Karen Hannah's Zoology background — whole-body biological systems analysis — means the assessment doesn't open with isolated symptom clusters.
It opens with how the autonomic nervous system is currently organizing the body. Where sustained activation has left measurable structural consequences. That's the starting point. Everything downstream follows from there.
That means reading resting muscle tone before a single adjustment is made.
Sustained psychological stress causes measurable electromyographical hyperactivity in the trapezius muscles — elevated resting electrical activity that most intake forms never ask about and most protocols never look for. Walk in with shoulders that are already electrically overloaded, and the assessment has to account for that before anything else happens.
Patients whose bodies show physical signs your body is stuck in threat mode need a care plan built around those specific layers — not a generic adjustment sequence that treats every nervous system the same.
The HPA axis gets assessed indirectly through what the patient actually reports: sleep quality, recovery rate, how fast tension returns after treatment.
Chronically high cortisol levels contribute directly to sustained muscle fiber contraction. When someone describes tension that's back within days of an adjustment, that's not a treatment failure. It's clinical data about a cortisol cycle that's still running — and that data changes the care plan.
Shockwave therapy becomes relevant when trigger points have calcified past the reach of standard soft tissue work. That determination comes from the assessment. Not from a service menu.
This Approach Is Not for Everyone
This approach isn't for everyone.
Not a disclaimer. A clinical reality worth saying out loud before you book.
If you're looking for a provider who'll replicate exactly what your last chiropractor did, this isn't that practice.
The assessment drives the care plan here — not your previous provider's sequence, not a front-desk intake form, and not a session count decided before the evaluation is finished. The patient who arrives expecting a specific protocol before any clinical picture is established will find this frustrating.
That frustration is useful information for both sides.
This is built for patients whose nervous systems are genuinely locked — whose tension keeps returning regardless of what they've already tried, and who want to understand what's actually driving the cycle, not just manage the output.
If you've been told it's stress and to relax, and that answer hasn't changed anything — the assessment is where a different conversation starts.
| Assessment Variable | What It Reveals | Why It Changes the Care Plan |
|---|---|---|
| Resting muscle electrical activity | Whether the trapezius and surrounding muscle groups are maintaining elevated tone even at baseline — before any movement or provocation | If resting tone is already overloaded, the care plan must address the autonomic driver first; adjusting into a chronically contracted muscle without that context produces short-term relief with rapid regression |
| Spinal joint mobility and restriction pattern | Which specific joints have lost normal range of motion and whether the restriction pattern is symmetrical or asymmetrical — asymmetry points to stress-locked muscle pull rather than structural injury | Asymmetric restriction changes both the sequence and the target of care; a bilateral protocol applied to a unilateral problem doesn't resolve the mechanical imbalance |
| Tension return rate between sessions | How quickly muscular tightness re-establishes itself after treatment — days versus weeks signals whether the cortisol cycle is still actively driving contraction | Rapid return of tension is clinical data, not treatment failure; it shifts the care plan toward addressing the HPA-axis feedback pattern rather than repeating the same soft tissue work |
| Sleep quality and recovery rate | Whether the autonomic nervous system is downregulating during rest or maintaining sympathetic activation overnight — poor sleep and slow recovery indicate the system isn't completing its off-cycle | A nervous system that can't power down at night requires a different care cadence; spacing sessions to allow genuine recovery windows becomes a clinical decision, not a scheduling preference |
| Patient-reported symptom pattern and history | What the patient actually reports — not what a diagnosis code anticipates — including which previous interventions helped, which didn't, and how long tension has been present as a baseline rather than an episode | The reported pattern distinguishes an acute stress response from a chronically locked nervous system; that distinction determines whether the care plan is short-course correction or a structured cycle of reassessment and adjustment |
Frequently Asked Questions
These are the questions people carry after being told "it's stress" — and that answer didn't move anything.
Not abstract. Biological. And each one has a specific answer.
Why does mental stress cause physical muscle pain in my neck and shoulders?
The stress response doesn't stay in the brain. The moment the autonomic nervous system reads a threat — real or perceived — it sends a cascade of signals directly into the body's muscular and vascular systems.
Sustained psychological stress causes measurable electromyographical hyperactivity in the trapezius muscles. That's elevated resting electrical activity in the exact muscles that hold your neck and shoulders up. The nervous system isn't signaling tension metaphorically. It's sending a contraction signal on repeat — long enough that the muscles can no longer fully release.
The pain is the output. Not the problem. The problem is the signal that won't stop.
What is the biological link between chronic stress and physical misalignment?
Sustained sympathetic activation causes vasoconstriction in peripheral muscle groups. Less blood flow. Less oxygen. Metabolic waste builds up faster than it clears — and that accumulation at the tissue level is what creates trigger points.
The HPA axis compounds it. Chronically high cortisol levels contribute directly to sustained muscle fiber contraction. The joints those muscles attach to gradually lose their normal range of motion.
The misalignment isn't the starting point. It's the structural record of how long the nervous system has been locked.
How does the nervous system lock skeletal muscles into a state of chronic spasm?
HPA-axis dysregulation directly correlates with somatic pain severity. The hypothalamic-pituitary-adrenal pathway keeps the cortisol signal running well after the original stressor disappears — and cortisol tells muscle fibers to stay contracted.
The spasm isn't a separate event from the stress. It's the end state of a nervous system that's been signaling threat long enough that elevated muscle tone has become the new resting baseline.
The body doesn't treat that as a problem. It treats it as normal. The muscles aren't misfiring — they're doing exactly what the nervous system keeps telling them to do.
Can targeted chiropractic care break the biological feedback loop of stress-related tension?
Yes — but only when the assessment identifies what's actually locked, not what a diagnosis code says should be there.
CDC research links chronic work-related mental stress to a statistically higher risk of physical musculoskeletal disorders. By the time those disorders show up, the nervous system has already left physical evidence throughout the body: restricted joints, elevated resting muscle tone, autonomic patterns keeping the whole loop running.
An individualized assessment reads that physical state. A care plan built from it — not from a generic protocol — addresses the specific layers maintaining the feedback loop.
The goal isn't to manage the tension. It's to interrupt the signal generating it.
Why don't standard stretching and relaxation techniques resolve chronic somatic tension?
Because the lock isn't cognitive. Stretching addresses muscle length. Relaxation techniques address mental state. Neither one changes the underlying autonomic activation maintaining the spasm.
Decreased oxygen delivery from sustained sympathetic vasoconstriction accelerates metabolic waste buildup at the tissue level — and a breathing exercise doesn't restore microcirculation to those fibers. Prolonged physical stress also reduces the body's natural capacity to repair micro-tears in soft tissue. Stretching a muscle that's been oxygen-deprived and chemically loaded doesn't clear that chemistry. It just moves it.
The sensor stays stuck. The alarm keeps firing not because the danger is real — but because the off-switch is broken. And the off-switch isn't in the mind.
The Alarm Doesn't Turn Off on Its Own
The car alarm is still blaring.
Not because the threat is present. Because the sensor never received the signal that it was gone. That's the biological reality underneath every patient who describes tension that keeps coming back — shoulders still tight the morning after they did everything right, sleep that won't stay fixed, a neck that locks up before noon on a Tuesday.
The off-switch isn't in the mind. It's in the physical structure the nervous system is reading.
A quieter environment doesn't reset a stuck sensor. Neither does a breathing exercise, a week off, or the same adjustment sequence run on every patient regardless of what their nervous system is actually doing.
What resets it is an assessment that reads the physical state the nervous system is in — resting muscle tone, restricted joints, the autonomic patterns holding the lock — and a care plan built specifically around those layers. Not a template. A response.
That's the structural intervention that turns the alarm off. That's what Touch of Wellness Chiropractic is built to do.
Stress-related tension isn't a mental weakness. It's a biological systems failure — and it has a physical address.
The alarm keeps firing not because the danger is real — but because the off-switch is broken. And a broken switch doesn't care how hard you breathe or how many days you take off.
If your body has been stuck in threat mode long enough to build structural evidence of it, the question isn't whether you should relax. The question is whether anyone has actually looked at what's locked.
That off-switch doesn't reset on its own. If the tension keeps returning no matter what you've tried, the next step isn't another strategy — it's a physical assessment that finds what's actually locked.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet