
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
The Best Sleeping Positions for Herniated Disc Recovery
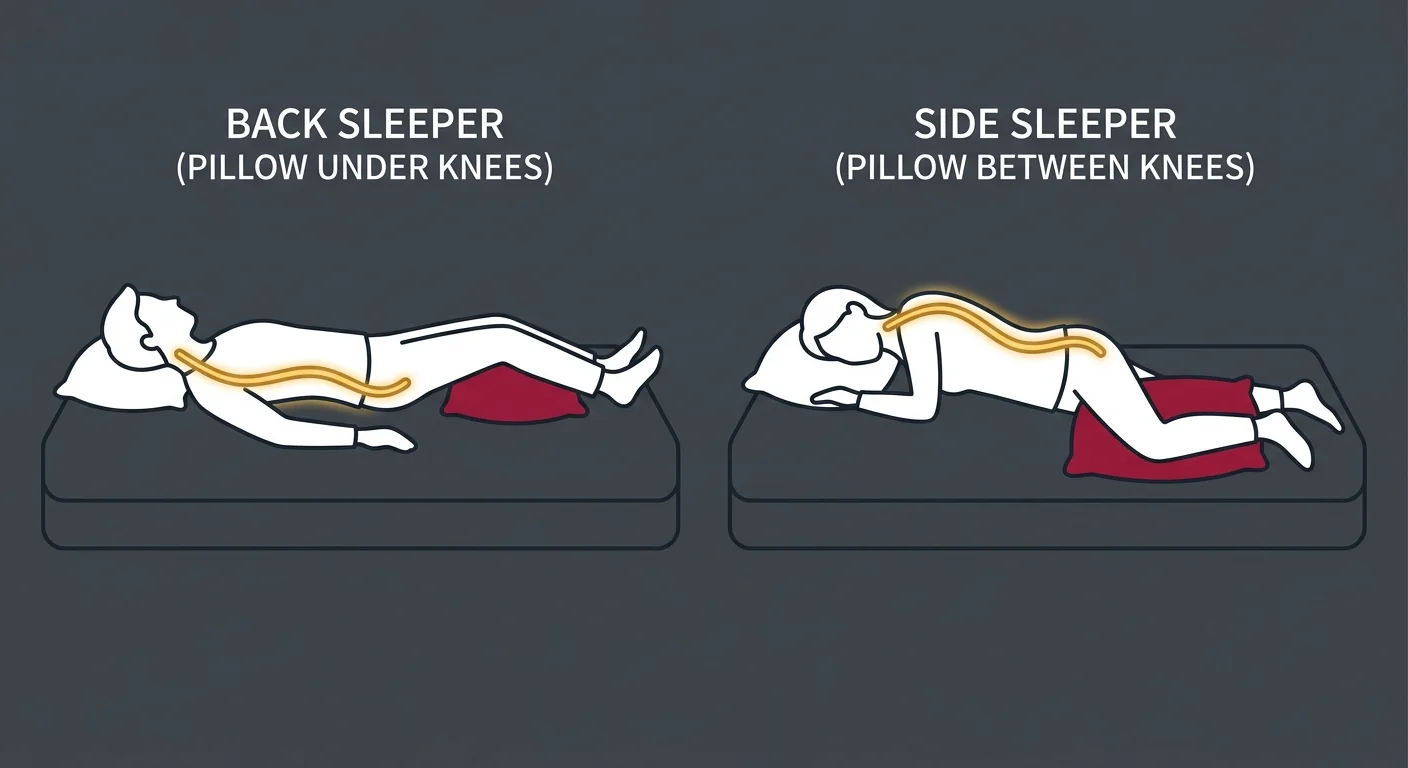
The best sleeping positions for herniated disc recovery maintain the natural curve of your spine and minimize pressure on the affected spinal nerves. The two most recommended positions are sleeping on your back with a pillow under your knees and sleeping on your side with a pillow between your knees. Both positions work by keeping your spine in neutral alignment, which reduces the mechanical stress on the herniated disc and prevents nerve root irritation while you sleep.
Sleeping on your back with a pillow under your knees preserves the lumbar curve and distributes your body weight evenly across the mattress. This position prevents the spine from flattening into the surface, which would otherwise increase pressure on the disc and the nerve it's compressing. Sleeping on your side with a pillow between your knees keeps your hips, pelvis, and spine stacked in alignment, preventing the top leg from pulling your spine out of position and twisting the lower back.
The worst position for herniated disc recovery is sleeping on your stomach. Stomach sleeping flattens the natural lumbar curve, forcing your lower back into extension for hours at a time. It also requires you to turn your head to one side to breathe, which twists your cervical spine and can create additional nerve tension. This combination of flattening and twisting creates the exact mechanical stress that aggravates disc herniations and delays healing.
These positions are not arbitrary comfort preferences. They are structural solutions to a mechanical problem. When a disc is herniated, it's bulging into the space where a spinal nerve exits the vertebral column. Any posture that increases pressure on that disc or pulls the nerve taut will produce pain and slow recovery. The right sleeping position removes that pressure and gives the nervous system the quiet, aligned environment it needs to begin healing overnight without being constantly re-irritated by poor spinal positioning.
Last Updated: April 30, 2026
- Why Sleeping Position Matters for Disc Recovery
- The Two Best Sleeping Positions for Herniated Discs
- Why Stomach Sleeping Is the Worst Position
- Pillow Placement Strategies to Support Recovery
- What to Do If the Right Position Still Causes Pain
- The Mattress Question: Does It Actually Matter?
- How to Get In and Out of Bed Without Triggering Pain
- Frequently Asked Questions
- Conclusion
Why Sleeping Position Matters for Disc Recovery
Most people dealing with a herniated disc have tried the pillow trick. Some got relief for a night. Most didn't.
That's not because the advice is bad. It's because stacking more pillows doesn't address why your disc herniated in the first place.
Your spine doesn't clock out at bedtime. The nervous system runs the entire recovery process while you're lying there. If you're holding a position that keeps compressing the nerve or twisting the disc, you're spending eight hours fighting against your own structure instead of letting it heal. That's the mechanical reality most online advice skips.
Your Spine Doesn't Stop Working While You Sleep
Inflammation regulation. Tissue repair. Muscle tension release. All of that happens while you're asleep, and it all depends on the nervous system having a clear signal pathway from brain to injury site and back.
When your spine's misaligned—even slightly—the nerve that's already compressed by the herniated disc gets additional pressure from poor positioning. That's not just uncomfortable. It's mechanically blocking the healing signals from getting through.
The right sleeping position isn't about comfort. It's about getting the interference out of the way so your body can do what it's designed to do overnight.
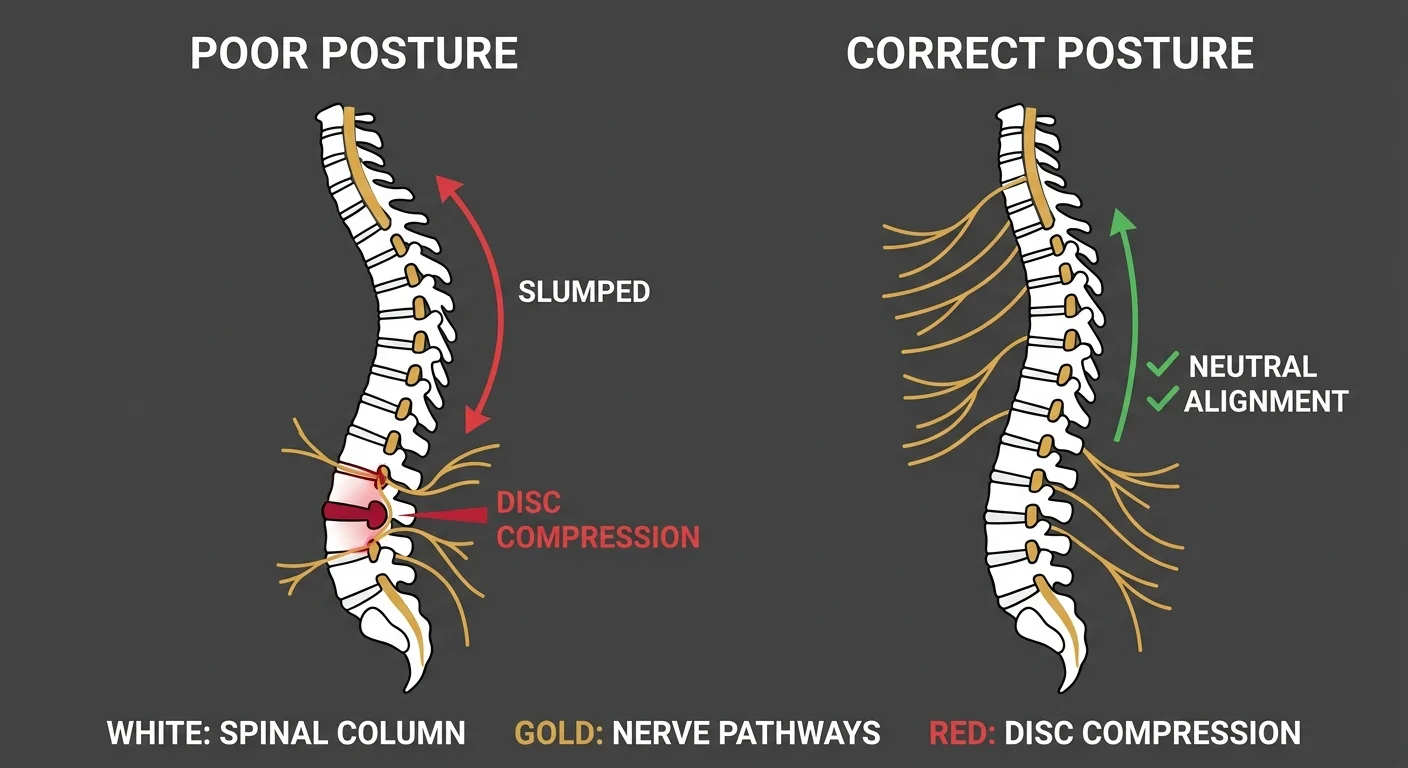
The Mechanical Reality of Disc Herniation
A herniated disc means the soft inner material of the disc has pushed through the outer ring and is now sitting in the space where a spinal nerve exits the vertebral column.
That nerve's trying to transmit signals between your brain and the rest of your body. When the disc presses on it, the signal gets disrupted. You feel that disruption as pain, numbness, tingling, or weakness—depending on which nerve and how much pressure.
Every position you hold either increases or decreases that pressure. If your sleeping position flattens your lumbar curve or twists your spine, you're adding hours of continuous stress to a nerve that's already compromised. According to the Mayo Clinic, one of the most critical recommendations for managing a herniated disc is avoiding positions that worsen nerve compression—and stomach sleeping is specifically flagged as problematic.
That's why people wake up worse than when they went to bed. Not bad luck. Mechanics.
Why "Just Use More Pillows" Doesn't Always Work
You've read the lists. Back sleeping with a pillow under your knees. Side sleeping with a pillow between. Maybe you tried it.
And it helped—for a week. Then the pain came back.
That's not because the pillow advice is wrong. It's because pillow placement addresses a symptom, not the cause.
The disc didn't herniate because you slept wrong. You slept wrong because the disc herniated—and probably because there was already a structural issue creating the conditions for that herniation in the first place. Most herniated discs don't appear out of nowhere. They're the result of repetitive stress, spinal misalignment, or compensatory movement patterns that've been building for months or years.
Changing your sleeping position removes one source of mechanical irritation. That's valuable. But if the underlying spinal dysfunction's still there—if your gait's off, if one hip's higher than the other, if your pelvis is rotated—you're just managing the symptom while the root cause keeps working in the background.
That's the gap between a tip and a care plan. One gives you temporary relief. The other stops the problem from coming back.
| What You've Tried | Why It Helped Temporarily | Why It Stopped Working | What's Actually Happening |
|---|---|---|---|
| Extra pillows under knees | Reduced lumbar extension and disc pressure for a few nights | Underlying spinal misalignment kept reloading the disc during the day | The disc's being compressed by a structural issue that doesn't go away when you adjust your pillows |
| Sleeping on your side | Prevented spinal twist and kept hips aligned temporarily | Muscle compensation patterns during the day pulled the spine back out of alignment | Your body's compensating for a pelvic or spinal imbalance that isn't being addressed |
| Firm mattress | Provided better support and reduced sagging initially | Disc continued to herniate because the root cause—nerve compression or spinal dysfunction—wasn't corrected | The mattress isn't the problem; the herniation's being driven by a movement or alignment issue that happens when you're awake |
| Sleeping in a recliner | Reduced pressure on the lower back by keeping hips and knees flexed | Created new problems in the thoracic spine and neck from prolonged semi-upright positioning | You're trading one mechanical stress for another without addressing the disc herniation itself |
The Two Best Sleeping Positions for Herniated Discs
These two positions work because they maintain the natural curves of your spine without forcing it into flexion, extension, or rotation.
That's not a preference. That's biomechanics.
Back Sleeping with Knee Support
Sleeping on your back with a pillow under your knees keeps your lumbar spine in its natural curve.
Without the pillow, your lower back flattens into the mattress. That flattening increases pressure on the disc and the nerve root it's compressing. The pillow lifts your knees just enough to tilt your pelvis back slightly, which restores the lumbar curve and takes the load off the disc.
- Preserves the natural lumbar curve — When your knees are elevated, your pelvis tilts posteriorly. That tilt reduces the arch in your lower back and distributes pressure evenly across the entire lumbar spine instead of concentrating it at the herniation site.
- Distributes weight evenly — Back sleeping spreads your body weight across the largest surface area, preventing pressure points from forming. This is especially important if the herniation's in the lower lumbar region where most body weight concentrates when lying flat.
- Keeps the pelvis neutral — A neutral pelvis means your hips aren't rotating or tilting in a way that'd pull the lumbar spine out of alignment. That stability's critical when the goal is to keep the disc from being mechanically stressed for eight hours straight.
Johns Hopkins Medicine specifically recommends back sleeping with knee support as one of the most effective ways to relieve pressure on a herniated disc overnight.
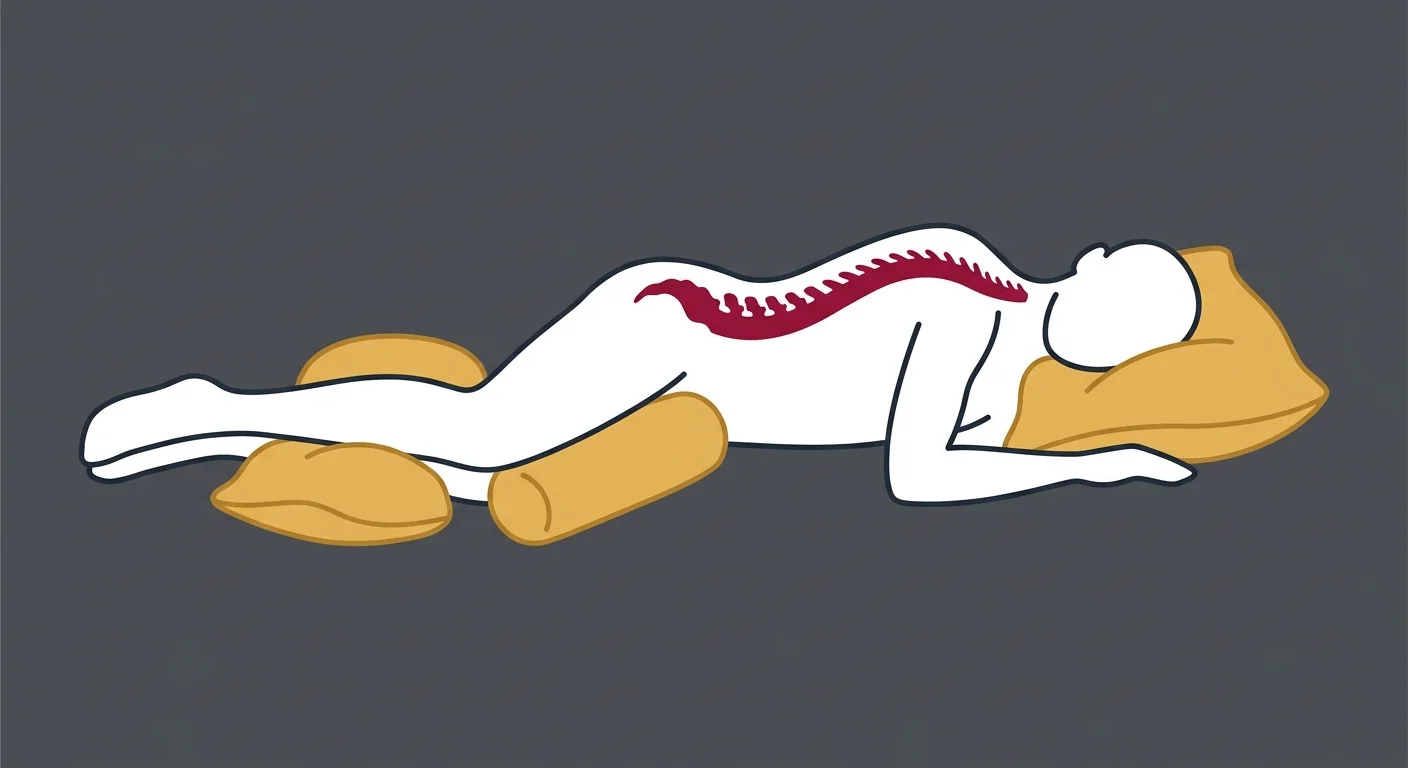
Side Sleeping with Pillow Between Knees
Side sleeping keeps your spine in a straight line from your neck to your tailbone—as long as you've got a pillow between your knees.
Without the pillow, your top leg drops down toward the mattress. That drop pulls your pelvis into rotation, which twists your lumbar spine. Even a small twist increases pressure on the disc and the nerve it's already compressing.
The pillow between your knees keeps your top leg level with your bottom leg. That keeps your hips stacked and prevents your spine from rotating.
- Prevents hip drop and spinal twist — When your top leg's supported, your pelvis stays level. A level pelvis means your lumbar spine isn't being twisted or side-bent, which is exactly what you need when a disc's already herniated and pressing on a nerve.
- Keeps the top leg from pulling the spine out of alignment — Gravity pulls your top leg down. That pull translates directly into rotational stress on your lower back. The pillow counters that gravity and keeps your spine neutral.
- Reduces pressure on the SI joint — The sacroiliac joint connects your pelvis to your spine. When your pelvis rotates, the SI joint absorbs that stress. If the SI joint's already irritated or misaligned, that added stress can create additional pain that mimics or worsens disc-related symptoms.
Side sleeping also allows you to curl slightly into a fetal position if needed, which can open up the space between the vertebrae and reduce compression on the nerve root. That's why many people with sciatica instinctively curl up on their side when the pain flares—it's a natural response to mechanical pressure.
Understanding how nervous system regulation works during sleep helps explain why proper alignment matters so much for recovery. Your body can't regulate inflammation or repair tissue effectively when the nervous system's constantly responding to mechanical irritation.
| Position | Primary Benefit | When It Works Best | Common Mistake |
|---|---|---|---|
| Back sleeping with pillow under knees | Preserves lumbar curve and distributes weight evenly | Best for central disc herniations and patients who naturally prefer back sleeping | Using a pillow that's too thick, which hyperflexes the hips and flattens the curve anyway |
| Side sleeping with pillow between knees | Prevents spinal rotation and keeps pelvis level | Best for lateral disc herniations and patients with sciatica radiating down one leg | Not using a thick enough pillow, allowing the top leg to drop and rotate the spine |
| Fetal position (side sleeping with knees drawn up) | Opens intervertebral space and reduces nerve compression | Best for acute flare-ups when even slight pressure causes radiating pain | Curling too tightly, which can create thoracic spine stiffness and new compensation patterns |
Why Stomach Sleeping Is the Worst Position

Stomach sleeping does two things that directly worsen a herniated disc: it flattens your lumbar curve and forces your neck into rotation for hours.
Both of those are the exact mechanical stresses you're trying to avoid.
It Flattens Your Lumbar Curve
When you lie face-down, your lower back's pressed into extension. The natural curve of your lumbar spine is flattened—or even reversed—depending on how soft your mattress is.
That flattening increases pressure on the anterior portion of the disc. If the herniation's already pushing backward into the spinal canal, flattening the curve pushes it even further into the nerve. You wake up with more pain because you spent the entire night mechanically loading the exact structure that's injured.
The University of Rochester Medical Center explains that stomach sleeping eliminates the natural lumbar curve and forces the spine into a position that increases stress on the discs and facet joints. For someone with a herniated disc, that's not just uncomfortable—it's actively preventing recovery.
It Forces Your Neck Into Rotation for Hours
You can't breathe face-down into a mattress. So you turn your head to one side.
That rotation pulls the cervical spine out of alignment. If the herniation's in your lower back, you might think your neck position doesn't matter. But the spine's a continuous chain. Cervical misalignment creates compensatory tension all the way down through the thoracic and lumbar regions.
Even if your herniation's isolated to the lumbar spine, that cervical rotation's adding mechanical stress to the entire system. Your body's trying to stabilize an unstable structure. That takes muscular effort. Muscular effort creates tension. Tension restricts blood flow and lymphatic drainage, both of which are critical for inflammation regulation and tissue repair.
You're not just sleeping wrong. You're forcing your body to work against itself for eight hours.
The "Transitional Stomach Sleeper" Problem
Some people don't start the night on their stomach. They start on their side or back—pillow positioned correctly, spine in neutral—and then roll onto their stomach at some point during the night.
They wake up in pain and assume the pillows didn't work. But the pillows did work—until they unconsciously moved into the position that undid all of it.
If you're a transitional stomach sleeper, the solution isn't just pillow placement. It's figuring out why your body's seeking that position in the first place. Sometimes it's habit. Sometimes it's because the side or back position isn't comfortable due to an unresolved structural issue—tight hip flexors, rotated pelvis, thoracic stiffness.
That's where a clinical assessment becomes necessary. You can't fix a movement pattern you're not aware of by reading an article. You need someone to watch how your body's compensating and build a plan around what's actually happening.
| What Happens | Lumbar Curve | Nerve Pressure | Neck Position |
|---|---|---|---|
| Back sleeping with pillow under knees | Natural curve maintained | Minimal—disc space preserved | Neutral, no rotation |
| Side sleeping with pillow between knees | Neutral alignment maintained | Minimal—spine stays straight | Neutral or slight side bend |
| Stomach sleeping | Flattened or reversed into extension | Maximal—disc pushed further into nerve | Rotated 90 degrees for hours |
| No pillow support (any position) | Collapses into whatever shape the mattress allows | Variable—often high due to poor alignment | Often hyperextended or side-bent |
Pillow Placement Strategies to Support Recovery
Pillow placement isn't about comfort. It's about creating the structural support your spine needs to stay in neutral alignment for eight hours.
Get the placement wrong and you're just adding more mechanical stress.
Under the Knees for Back Sleepers
The pillow under your knees should be thick enough to create a visible bend in your hips and knees—not flat, not a token gesture.
If the pillow's too thin, your legs'll straighten out during the night and your lumbar curve'll flatten. If the pillow's too thick, your hips'll be hyperflexed and your lower back'll round into flexion, which can increase pressure on the posterior disc and worsen nerve compression.
The right height is when your knees are bent at about 30 to 45 degrees. That angle tilts your pelvis just enough to restore the lumbar curve without overflexing the hips.
Use a standard bed pillow or a wedge bolster—doesn't matter which. What matters is height and firmness. A pillow that collapses under the weight of your legs isn't doing anything.
Between the Knees for Side Sleepers
For side sleepers, the pillow between your knees needs to be thick enough to keep your top leg level with your bottom leg.
A standard pillow works for most people. A full-length body pillow works better if you also need support for your top arm or if you tend to roll forward during the night. The body pillow acts as a physical barrier that prevents you from rotating your torso toward the mattress.
The goal is to keep your hips stacked. If your top hip's dropping forward or backward, your pelvis is rotating. Pelvic rotation pulls the lumbar spine into a twist. That twist increases disc pressure and nerve irritation.
If you wake up with your pillow on the floor, you need a thicker pillow or a body pillow that's harder to dislodge.
If you're not sure whether your pelvis is level, have someone take a photo of you lying on your side with the pillow in place. Your hips should form a straight vertical line. If the top hip's tilted forward or backward, adjust the pillow height.
Knowing the early signs of a bulging disc can help you catch the problem before it becomes a full herniation. But once the disc's herniated, pillow placement's part of the recovery strategy—not the whole strategy.
Head and Neck Pillow Height
Your head pillow controls the alignment of your cervical spine. Your cervical spine's directly connected to your thoracic spine. Your thoracic spine's directly connected to your lumbar spine.
If your head pillow's too high, your neck's flexed forward for hours. That forward flexion creates tension in the upper traps and cervical paraspinals, which translates down through the thoracic spine and eventually affects lumbar mechanics.
If your head pillow's too low, your neck's extended backward. That extension compresses the facet joints in the cervical spine and creates compensatory tension in the lower back.
The right height keeps your nose in line with the center of your body when you're on your back, and keeps your head level with your spine when you're on your side.
Most people use a pillow that's too high because they've been conditioned to think "more support" is better. More isn't better. Neutral is better.
The Cleveland Clinic provides detailed guidance on pillow placement for patients with sciatica, emphasizing that proper support of the head, knees, and hips works as a system—not as isolated adjustments.
What to Do If the Right Position Still Causes Pain

You've changed your position. You've added the pillows. You're doing everything the articles say to do.
And it's still not working.
That's not failure. That's information.
If the right sleeping position doesn't reduce your pain, it means the position isn't the main problem. The herniation itself—and whatever caused it—is the main problem. Sleeping position supports recovery. It doesn't create recovery.
Sleeping Position Supports Recovery — It Doesn't Create Recovery
Most herniated discs don't appear out of nowhere.
They're the result of repetitive stress, compensatory movement patterns, spinal misalignment, or muscular imbalances that've been building for months or years. The disc finally gives out under the accumulated load. The herniation's the breaking point, not the starting point.
Changing your sleeping position removes one source of mechanical irritation. That's valuable. But if the underlying dysfunction's still there—if your gait's off, if one hip's higher than the other, if your pelvis is rotated—you're managing a symptom while the root cause keeps working in the background.
That's the difference between a tip and a care plan. A tip gives you temporary relief. A care plan addresses why the disc herniated in the first place and builds a strategy to prevent it from happening again.
Chiropractic care is designed to identify and correct the structural dysfunctions that create the conditions for disc herniation. Adjusting your sleeping position's part of that plan. But it's not the whole plan.
If you're doing everything right at night and still waking up in pain, that's the signal that the daytime mechanics are still the problem.
This is where most people fall into the Plan Picker trap. They change their sleeping position but ignore the fact that they're still sitting in a twisted posture at work for eight hours. Or they're still limping because one leg hurts. Or they're still compensating for a hip that doesn't move correctly.
Partial commitment produces partial results. That's not a character flaw. That's mechanics.
When Pain Moves or Changes with Position
If your pain shifts from your lower back to your hip when you change positions, that's not a bad sign. That's your nervous system responding to a change in mechanical load.
Pain that moves is different from pain that stays in one place. Pain that stays in one place is usually being driven by a single structure under constant mechanical stress. Pain that moves is usually being driven by multiple structures compensating for each other.
When you change your sleeping position, you're redistributing the load across your spine. If the pain moves from your lower back to your hip, it means your hip was already compensating for the lumbar dysfunction. The sleeping position exposed that compensation instead of masking it.
That's useful information. It tells you the herniation isn't the only issue. There's a chain of dysfunction, and each link in that chain needs to be addressed individually.
Nerve pain and muscular pain feel different. Nerve pain's sharp, electric, radiating. Muscular pain's dull, achy, localized. If your pain's moving and changing quality, you're dealing with both—and that requires a more comprehensive approach than pillow placement.
According to Medical News Today, when sleeping position changes produce inconsistent results, it often indicates that multiple contributing factors—such as muscle tension, inflammation, and nerve compression—are all present and need to be addressed together.
The Role of Inflammation vs. Mechanical Pressure
Sometimes the pain persists even in the right position because the problem isn't mechanical anymore. It's inflammatory.
When a disc herniates, the inner disc material that leaks out into the spinal canal contains chemical irritants that trigger an inflammatory response. That inflammation can persist for weeks even after the mechanical pressure's been reduced.
Sleeping in the right position removes the mechanical stress. It doesn't remove the inflammation. That's why some people follow all the positioning advice and still wake up in pain for the first week or two. The nervous system's still responding to the chemical irritation, not just the physical compression.
The inflammatory phase is part of the healing process. Your body's sending immune cells to clean up the damaged tissue and repair the area. That process produces swelling, and swelling produces pressure, and pressure produces pain.
The timeline matters. If you've been sleeping in the right position for a few days and you're still in pain, that's expected. If you've been sleeping in the right position for three weeks and the pain hasn't changed at all, that's a different situation. That's when you need to ask whether the disc is the only issue or whether there's a structural dysfunction that's preventing the inflammation from resolving.
Understanding why sciatica keeps coming back is critical here. If the herniation's in the lumbar spine and you're experiencing radiating leg pain, the sleeping position's only part of the equation. The nerve pathway needs to be decompressed, and the structural cause of the herniation needs to be corrected.
The Mattress Question: Does It Actually Matter?
Yes. But not in the way most people think.
Your mattress doesn't cause a herniated disc. But a worn-out or poorly matched mattress can prevent recovery by failing to support your spine in neutral alignment overnight.
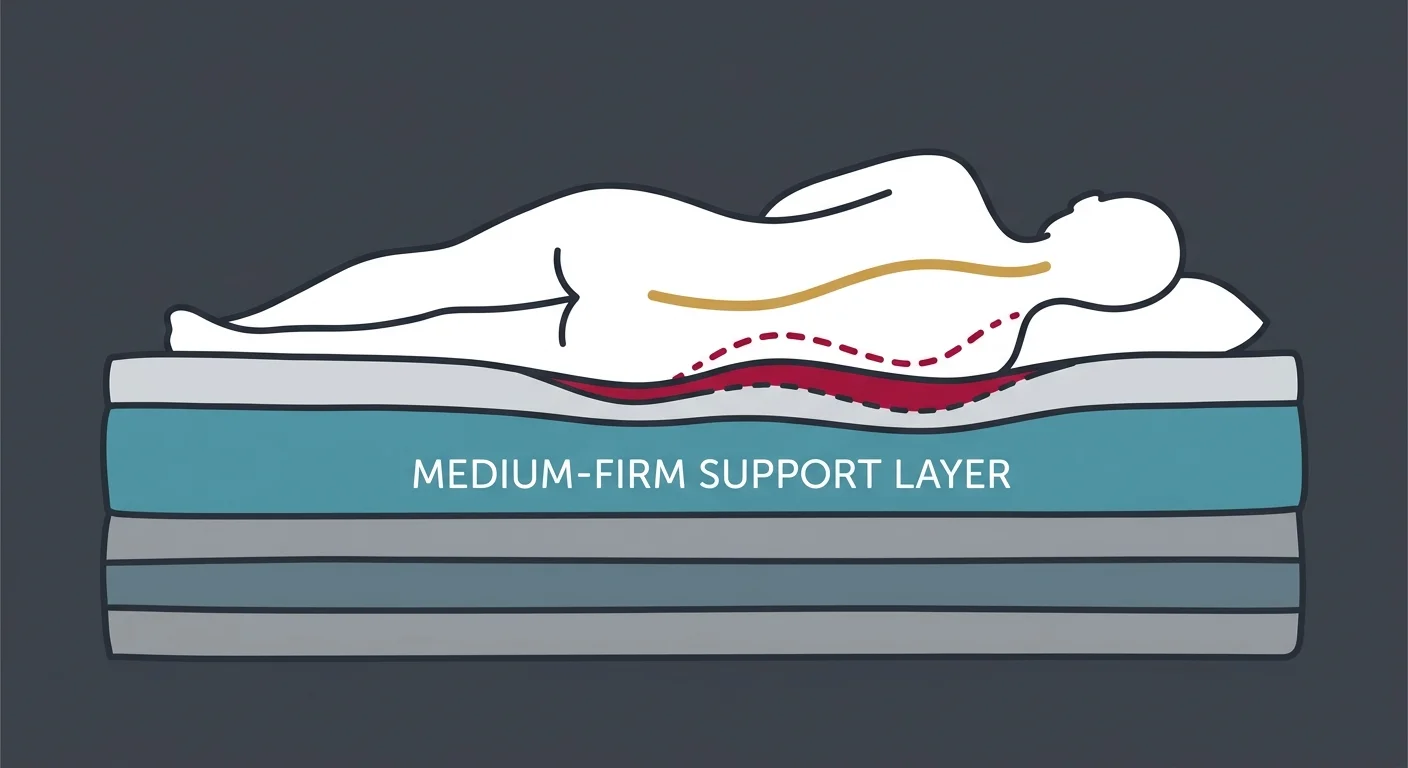
Medium-Firm Is the Target
Medium-firm means the mattress resists your body weight enough to keep your spine from sagging, but gives enough to accommodate the natural curves of your body.
A mattress that's too soft allows your hips and shoulders to sink too far into the surface. That creates a hammock effect where your spine bends in the middle. If you're on your back, your lumbar curve collapses. If you're on your side, your spine curves laterally instead of staying straight.
A mattress that's too hard doesn't accommodate the natural curves of your body at all. Your hips and shoulders can't sink in even slightly, which means your spine's forced to bridge the gap between those two high points. That creates pressure points and prevents your muscles from fully relaxing.
Medium-firm's the balance point. Your hips and shoulders sink in just enough to allow your spine to maintain its natural alignment without forcing it into flexion or extension.
The problem is that "medium-firm" is subjective. What feels medium-firm to a 150-pound person feels too soft to a 250-pound person. The industry doesn't have a universal firmness scale, so you can't rely on manufacturer labels alone.
The test: lie on your back. Slide your hand under your lower back. If there's a big gap—enough space to slide your hand through easily—the mattress is too firm. If there's no gap at all—if your lower back's pressed flat into the mattress—the mattress is too soft. If there's a small gap that your hand just barely fits into, that's about right.
The Floor Sleeping Myth
Sleeping on the floor isn't necessary for most people with a herniated disc.
Some people find temporary relief on a firm surface because their mattress was too soft and allowing their spine to sag. But a medium-firm mattress provides the same support without the discomfort of sleeping on a completely unyielding surface.
Floor sleeping works for a specific subset of people: those whose pain's being driven by excessive lumbar flexion due to a mattress that's collapsed or too soft. If that's you, the floor provides immediate feedback that your mattress is the problem.
But for most people, floor sleeping creates new problems. It doesn't accommodate the natural curves of your body at all, which means your muscles have to stay partially engaged all night to stabilize your spine. That prevents full relaxation and can create thoracic and cervical stiffness by morning.
If you're considering sleeping on the floor because your mattress isn't working, the real question is whether you need a firmer mattress or whether the mattress is fine and the disc herniation itself is the issue. Most of the time, it's the latter.
Floor sleeping's an extreme test, not a long-term solution.
When to Replace Your Mattress
A mattress that's more than 7 to 10 years old is probably past its functional lifespan, even if it doesn't look worn out.
The support layers compress over time. The surface may still look fine, but the core's no longer providing the resistance it did when it was new. That compression's gradual, so you don't notice it happening until you wake up one day and realize you're in more pain than you were a year ago.
The sagging test: lie on your back in the center of the mattress. Have someone look at you from the side. If your hips are visibly lower than your shoulders and knees—if there's a noticeable dip in the middle—the mattress has lost its structural integrity.
If your mattress is sagging, no amount of pillow adjustment'll fix the problem. You're fighting gravity and a collapsed support structure at the same time.
Replacing a mattress is expensive. But if the mattress is preventing your spine from staying in neutral alignment for eight hours a night, it's actively working against your recovery.
| Firmness Level | Spinal Support | Best For | Problem |
|---|---|---|---|
| Too Soft | Allows excessive sinking; spine sags into flexion | Very lightweight sleepers or those with no structural issues | Creates hammock effect; lumbar curve collapses, increasing disc pressure |
| Medium-Firm | Resists body weight while accommodating natural curves | Most people with herniated discs | Subjective—varies by body weight and mattress construction |
| Too Hard | No accommodation for body curves; forces spine to bridge gaps | No one—this is always a compensation | Creates pressure points; prevents muscle relaxation; can worsen nerve pain |
How to Get In and Out of Bed Without Triggering Pain
Most people trigger their herniated disc pain before they even get out of bed.
They sit straight up. They twist at the waist to reach for something. They swing their legs over the side while their torso's still flat.
All of those movements load the disc in exactly the way you're trying to avoid.
The Log Roll Technique
The log roll keeps your spine in neutral alignment during the transition from lying down to sitting up.
It's called a log roll because you move your entire body as a single unit—no twisting, no bending, no segmental movement at the spine.
- Step 1: Roll to your side — From your back, bend your knees slightly and roll your entire body onto your side in one motion. Your shoulders, hips, and knees should move together. Don't twist your torso to initiate the roll. Let your legs lead and your torso follows.
- Step 2: Swing your legs over the edge — Once you're on your side, pause. Then swing both legs over the edge of the bed together. Your knees should drop toward the floor while your torso's still lying on its side. This uses the weight of your legs to help pull your torso upright without requiring you to engage your lower back muscles.
- Step 3: Push up with your arms — As your legs drop, use your arms to push your torso up to a sitting position. Your spine stays straight the entire time. You're using your arms and the momentum of your legs to do the work—not your lower back.
The reverse process applies when getting into bed. Sit on the edge of the bed. Lower your torso to your side while lifting your legs onto the mattress. Then roll onto your back as a single unit.
This feels awkward at first. Most people've been sitting straight up out of bed their entire lives. But sitting straight up from a lying position requires your hip flexors and lower back muscles to do all the work. When you've got a herniated disc, that contraction increases pressure on the disc and can trigger immediate pain.
What Not to Do
Don't sit straight up from a lying position. That's a sit-up. Sit-ups load the lumbar spine in flexion, which is exactly what you're trying to avoid.
Don't twist your torso to reach for something on the nightstand. If you need to reach for something, roll onto your side first. Then reach. Then roll back. Twisting under load is how most people re-injure a disc that was starting to heal.
Don't reach overhead while lying on your back. Reaching overhead arches your lower back into extension. If the disc's already herniated posteriorly, that extension increases pressure on the nerve.
These movements seem minor. But when a disc's herniated and a nerve's compressed, even small mechanical stresses add up over the course of a day.
One bad movement doesn't ruin your recovery. But repeating the same bad movement ten times a day for a week keeps the disc and nerve under constant irritation. That prevents healing and creates the conditions for the pain to become chronic.
The connection between chronic stress and back pain matters here too. If you're stressed, your muscles stay tense. Tense muscles don't move efficiently. Inefficient movement loads your spine asymmetrically. Asymmetric loading increases disc pressure. That's how a herniated disc that should've healed in six weeks turns into a problem that lasts six months.
Frequently Asked Questions
What is the absolute worst sleeping position for a herniated disc?
Stomach sleeping's the worst position because it forces your lumbar spine into extension and requires you to rotate your neck for hours to breathe.
The extension flattens or reverses your lumbar curve, which increases pressure on the anterior portion of the disc and pushes the herniation further into the spinal canal. The neck rotation creates compensatory tension throughout the entire spine, preventing your muscles from fully relaxing and restricting blood flow to the area.
If you're a stomach sleeper and you're not willing to change positions, the herniation'll take longer to heal. That's not an opinion. That's mechanics.
Can the right mattress help with herniated disc recovery?
Yes, but only if your current mattress is actively working against you.
A medium-firm mattress that keeps your spine in neutral alignment overnight supports recovery by removing one source of mechanical stress. But a new mattress doesn't correct the structural dysfunction that caused the herniation in the first place.
If your mattress is less than seven years old and passes the sagging test, replacing it probably won't change your pain level. If your mattress is sagging or too soft, replacing it might make a noticeable difference within the first week.
The mattress is part of the environment. It's not the treatment.
Why does my herniated disc pain feel worse at night?
Pain often feels worse at night because you're no longer distracted by work, conversations, or movement. Your brain's got nothing else to focus on, so the pain signal becomes the dominant input.
There's also a physiological component. When you lie down, fluid shifts back into the spinal discs. That fluid shift can temporarily increase disc pressure and nerve compression, especially in the first hour after you lie down. Inflammatory processes can also increase with inactivity, which is why some people feel stiff and sore when they first wake up even if they were fine during the day.
If your pain's consistently worse at night, it might not be the sleeping position. It might be inflammation that hasn't resolved yet, or it might be a structural issue that's being masked by movement during the day and exposed when you're lying still.
The New York Times notes that back and side sleeping are generally the most supportive positions for spinal health, but if pain persists regardless of position, the underlying issue often requires professional assessment rather than self-management alone.
How should I get in and out of bed with a herniated disc?
Use the log roll technique.
Roll onto your side as a single unit. Swing your legs over the edge of the bed while your torso's still on its side. Push up with your arms while your legs drop toward the floor. Your spine stays straight the entire time.
Don't sit straight up. Don't twist to reach for something. Don't arch your back to reach overhead. All of those movements load the disc and can trigger pain even if you were fine a minute ago.
Is it better to sleep on the floor for a herniated disc?
No, for most people.
Floor sleeping works if your mattress is too soft and allowing your spine to sag. But a medium-firm mattress provides the same support without the discomfort of a completely unyielding surface.
The floor doesn't accommodate the natural curves of your body at all. That means your muscles stay partially engaged all night to stabilize your spine. That prevents full relaxation and can create new problems in your thoracic spine and neck.
If you're considering sleeping on the floor, test it for one or two nights. If your pain improves, your mattress is the problem—not your sleeping position. Replace the mattress instead of sleeping on the floor long-term.
If I sleep in the right position, will my disc heal on its own?
Sleeping in the right position supports healing. It doesn't create healing.
A herniated disc can heal on its own if the mechanical stress that caused it's removed and the body's natural repair processes are allowed to work. But if the structural dysfunction that led to the herniation's still present—if your gait's off, if your pelvis is rotated, if one hip's higher than the other—sleeping in the right position only addresses part of the problem.
Most herniated discs don't appear out of nowhere. They're the result of accumulated stress over time. If you change your sleeping position but ignore the daytime mechanics that caused the herniation, you're managing a symptom while the root cause continues working in the background.
That's why some people change their sleeping position and feel better for a few weeks, then the pain comes back. The position helped. But it wasn't enough to stop the underlying dysfunction.
Learning how to maintain disc health after the acute phase is over is just as important as managing the pain during recovery. Prevention's a plan, not an accident.
How long does it take to see improvement from changing my sleeping position?
Some people feel better within the first night. Others take a week or two.
If the pain's being driven purely by mechanical compression—meaning the disc is pressing on the nerve and poor sleeping position's making it worse—you should feel at least some improvement within 48 hours of switching to a better position.
If the pain hasn't changed at all after a week, it means the sleeping position wasn't the main problem. The herniation itself, the inflammation, or the underlying structural dysfunction's the main driver. In that case, pillow adjustments and position changes are helpful but not sufficient.
Pain that improves for a few days and then plateaus usually means you've addressed one layer of the problem but there's another layer underneath that still needs attention.
Can I use a recliner instead of a bed?
A recliner can provide temporary relief if lying flat increases your pain, but it's not a long-term solution.
Recliners keep your hips and knees flexed, which reduces pressure on the lumbar spine. That's why some people with acute sciatica find relief in a recliner during the first few days of a flare-up.
But sleeping in a recliner for weeks creates new problems. Your thoracic spine stays rounded, your neck stays flexed forward, and your body never fully relaxes into a neutral position. That creates stiffness in the upper back and neck, which eventually adds to the total mechanical stress on your spine.
If a recliner's the only position that doesn't cause pain, that's important clinical information. It means the disc herniation's severe enough that even neutral positions are painful. That level of pain requires professional assessment—not indefinite recliner use.
Conclusion
The right sleeping position gives your nervous system the space it needs to work overnight without constant mechanical interference.
But sleeping position's part of a recovery strategy. It's not the strategy.
If you've changed your position and you're still waking up in pain, that's not failure. That's your body telling you the disc herniation isn't the only issue. The structural dysfunction that created the herniation's still there, and it's not going to resolve itself just because you adjusted your pillows.
Most herniated discs are the breaking point of a system that's been compensating for months or years. Changing your sleeping position removes one source of stress. But if your gait's off, if one hip's higher than the other, if your pelvis is rotated, if your core isn't stabilizing your spine during movement—those are the problems that allowed the disc to herniate in the first place.
You can't fix that with a pillow.
The nervous system runs everything. When a disc's herniated, nothing works right—and you feel that every night. What you don't need is another provider who hands you a pillow guide and calls it a care plan. Unexplained doesn't mean untreatable. It means no one's looked hard enough yet. That requires a proper clinical evaluation that looks at how your body's moving, where it's compensating, and what's been missed.
Sleeping in the right position's a tool. It's a good tool. But if the tool isn't producing results, that's the signal that the problem's bigger than the position—and it's time to stop managing symptoms and start addressing the cause.
If your herniated disc pain's waking you up every night and sleeping position changes aren't giving you the relief you expected, that's worth a real conversation.
A chiropractic assessment at Touch of Wellness Chiropractic doesn't start with a 12-month plan. It starts with figuring out why the disc herniated—not just where it hurts. Not a protocol. Not a generic timeline. A plan built from what your body's actually doing and what it needs to function again.
If you're in Morton, Peoria, or the surrounding area and you want to know what's driving your pain instead of just managing it, find out what your assessment looks like.
Proper sleeping position supports recovery. But if the root cause's still there, the pain keeps coming back. That's not bad luck. That's mechanics.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet