
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
5 Primary Signs of a Bulging Disc in Your Lower Back (And Why They Recur)
The primary signs of a bulging disc in the lower back aren't random aches that come and go for no reason. They're your nervous system sending clear signals that a structural problem is compressing a nerve root. That compression produces a pattern: deep, localized pain in the lower back that often radiates down one leg as sciatica, numbness or tingling in specific areas of the leg or foot, muscle weakness that shows up in precise movement patterns, and symptoms that worsen with sitting, bending, or twisting.
Here's what most people don't realize until they've cycled through multiple rounds of treatment that didn't stick: these symptoms recur because the underlying cause—the disc pressing on the nerve—was never addressed. You got relief because inflammation calmed down or muscle tension released temporarily. But the structural pressure remained. So the next time you bend wrong, sit too long, or lift something awkwardly, the nerve gets irritated again and the whole cycle restarts.
The frustration isn't that the pain came back. It's that no one explained why it came back or what needed to change to stop it from happening again. A bulging disc doesn't announce itself with vague discomfort. It produces specific, recognizable symptoms that map directly to which nerve root is being compressed and how severely. If you know what you're looking at, the pattern is clear. If you don't, you're left treating the symptom while the cause stays intact.
This article breaks down the five primary signs of a bulging disc in the lower back, explains why each one occurs, and clarifies why these symptoms keep returning when the root cause goes untreated. If you've been told your pain is unexplained, that it's just muscle strain, or that you need to wait and see if it gets better on its own—this is the conversation no one's had with you yet.
Last Updated: April 30, 2026
- What a Bulging Disc Actually Is (And Why the Term Gets Misused)
- Sign 1: Deep, Localized Lower Back Pain That Won't Resolve
- Sign 2: Radiating Pain Down One Leg (Sciatica)
- Sign 3: Numbness or Tingling in Specific Leg or Foot Zones
- Sign 4: Muscle Weakness in Precise Movement Patterns
- Sign 5: Symptoms That Worsen With Sitting, Bending, or Twisting
- Why These Signs Keep Coming Back (The Recurrence Problem)
- Frequently Asked Questions
- Conclusion
What a Bulging Disc Actually Is (And Why the Term Gets Misused)
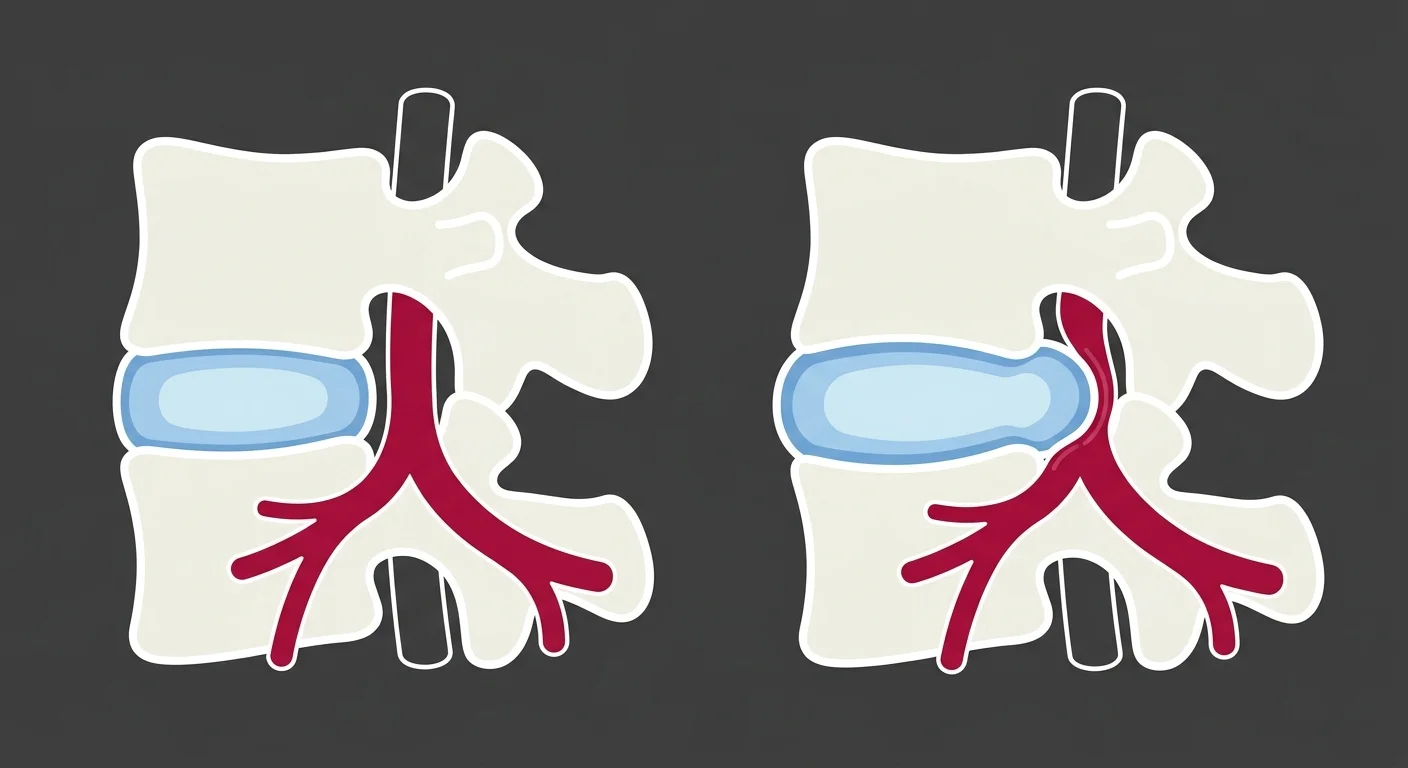
Most people are told they have a bulging disc without anyone explaining what that actually means—or why it matters. A bulging disc is exactly what it sounds like: the disc between two vertebrae swells outward, pushing past its normal boundary.
Think of it like an underinflated tire. The whole outer edge bulges evenly, creating pressure where it shouldn't be.
That's different from a herniated disc, where the outer layer cracks and the gel-like center leaks out. According to Medical News Today, a bulge is a contained protrusion—the disc material stays inside the outer wall. A herniation is a rupture. Both can compress nerves, but herniation is typically more severe.
Your spinal discs act as cushions between vertebrae. They absorb shock and allow your spine to bend and twist. When a disc bulges, it extends into the space where nerve roots exit the spinal column. That creates pressure on the nerve. And that pressure is what produces the five signs covered in this article.
The bulge itself doesn't always hurt. What hurts is the nerve compression. The National Institute of Neurological Disorders and Stroke explains that when the bulging disc material presses against a nerve root, it triggers inflammation and interferes with normal nerve signal transmission. That's when you start feeling pain, numbness, tingling, or weakness.
Why "Bulging Disc" Gets Used as a Catch-All Diagnosis
A lot of providers use "bulging disc" generically for any lower back pain that radiates into the leg. That creates confusion.
Not all lower back pain is disc-related. And not all disc bulges cause symptoms.
Studies show that many people have disc bulges visible on MRI but no pain at all. The bulge becomes clinically significant only when it compresses a nerve root enough to produce the specific patterns described in this article.
So when someone says "bulging disc," what you need to know is: which nerve is being compressed, how severely, and what's causing the compression to persist.
The Cookie-Cutter Protocol Problem
Most chiropractic offices run the same protocol on every lower back pain patient.
Walk in with sciatica, walk in with muscle strain, walk in with a suspected disc issue—you get the same sequence. When it doesn't work, they run it again. That's not a care plan. That's a template.
Disc symptoms require precise assessment of which nerve root is involved and how severely it's compressed. An L4 nerve compression produces different symptoms than an L5 or S1 compression. The care plan has to match the clinical picture—not a prebuilt protocol designed for maximum billing efficiency.
Individualized chiropractic care starts with what you actually report. Where does the pain radiate? What positions make it worse? Which movements trigger numbness? The answers to those questions determine the treatment—not a flowchart that treats every lumbar complaint the same way.
Sign 1: Deep, Localized Lower Back Pain That Won't Resolve

The first sign is a persistent, deep ache in your lower back that doesn't respond to stretching or rest the way muscle pain does.
This isn't soreness from overuse. It's a constant, nagging discomfort that stays in one spot. Sometimes it's dull. Sometimes it sharpens with certain movements. But it doesn't migrate around your back the way muscle strain does.
That localized pain comes from two sources. First, the bulging disc itself causes mechanical irritation to surrounding tissues. Second, when the disc presses on a nerve root, it triggers inflammation in that area. Mayo Clinic notes that this inflammation can persist even when you're at rest, which is why the pain lingers long after the activity that triggered it.
Why Rest and Pain Relievers Only Work Temporarily
Anti-inflammatory medication reduces swelling around the disc. That takes pressure off the nerve, and the pain improves. But the medication doesn't reposition the disc. It doesn't change the structural bulge that's compressing the nerve in the first place.
Rest works the same way.
When you lie down, you reduce the load on your spine. Disc pressure decreases. The nerve compression eases. You feel better.
Then you get up, sit for an hour, bend over to pick something up—and the pain returns. The structural cause is still there. You're managing the symptom, not fixing the source.
| Characteristic | Disc-Related Pain | Muscle Strain Pain |
|---|---|---|
| Pain Type | Deep, persistent ache; sharp with certain movements | Dull soreness; improves with gentle movement |
| Location | Stays in one specific spot in lower back | Can move or spread across multiple areas |
| Response to Rest | May improve temporarily but returns with activity | Usually resolves with adequate rest |
| Response to Stretching | Little to no relief; may worsen with certain positions | Often improves with appropriate stretching |
| Duration | Persists for weeks or months if untreated | Typically resolves within days to two weeks |
| Associated Symptoms | Often accompanied by leg symptoms (numbness, tingling, weakness) | Rarely involves symptoms below the back |
Sign 2: Radiating Pain Down One Leg (Sciatica)

Sciatica is nerve pain—not muscle pain.
It follows the path of the sciatic nerve: down your buttock, through the back of your thigh, sometimes into your calf and foot. The pain is often described as sharp, burning, or electric. Some people say it feels like a lightning bolt shooting down their leg.
This happens when the bulging disc compresses the nerve root that feeds into the sciatic nerve. The American Academy of Orthopaedic Surgeons explains that the sciatic nerve is formed by nerve roots exiting the lower lumbar and sacral spine—specifically L4, L5, and S1. When a disc at one of those levels bulges, it can irritate the nerve root and send pain signals down the entire length of the sciatic nerve.
That's why sciatica from a disc bulge is almost always one-sided. The disc typically bulges toward one side of the spinal canal, compressing the nerve root on that side only.
With individualized chiropractic care, the first step is identifying which nerve root is involved. That determines the treatment approach—because an L4 compression requires different positioning and adjustment strategies than an S1 compression.
Why the Pain Moves (And What That Movement Means)
Some days your sciatica is in your buttock. Other days it's in your calf. That's not random.
As the disc bulge changes position—swelling more, shifting slightly, or responding to inflammation—the degree of nerve compression changes. When the pressure is higher, the pain travels farther down the leg. When the pressure eases, the pain retreats back toward the buttock.
The location of the pain at any given moment maps to how much of the nerve is being compressed.
This is useful diagnostic information. It tells you whether the compression is worsening, improving, or staying the same.
| Nerve Root | Pain Location | Common Triggers |
|---|---|---|
| L4 | Front of thigh, inner shin, sometimes into inner ankle | Prolonged standing, walking uphill, extension-based movements |
| L5 | Outer thigh, outer calf, top of foot, big toe | Bending forward, sitting with poor posture, lifting with rounded back |
| S1 | Back of thigh, back of calf, outside of foot, little toe | Sitting for extended periods, especially in car seats or soft furniture |
Sign 3: Numbness or Tingling in Specific Leg or Foot Zones

Numbness and tingling from a bulging disc aren't vague sensations that drift around your leg. They follow dermatomal patterns—specific zones of skin supplied by a single nerve root.
An L5 nerve compression causes numbness on the top of your foot and big toe.
An S1 compression causes numbness on the outside of your foot and little toe. An L4 compression affects the inner shin and sometimes the inner ankle.
This precision is diagnostic. It tells you exactly which nerve root is being compressed. The National Institute of Neurological Disorders and Stroke notes that these dermatomal maps are consistent across patients, which is why trained providers can pinpoint the level of disc involvement based on where you're experiencing numbness.
If you're dealing with nerve-related symptoms, this is the starting point. The pattern of numbness reveals the structural problem. From there, the assessment focuses on what's causing that specific nerve root to be compressed and what needs to change to relieve it.
Why Numbness Is a Red Flag (Not Just an Inconvenience)
Numbness means the nerve isn't transmitting sensory signals correctly.
If that continues long enough, the nerve can sustain damage. Prolonged compression can lead to permanent sensory changes or motor weakness. This is why "wait and see" is not a neutral recommendation when numbness is involved.
The longer the nerve is compressed, the harder it is to restore full function.
Early intervention—addressing the disc pressure before the nerve degenerates—produces better outcomes than waiting until the numbness has been present for months.
- Immediate numbness (within days) — Usually reversible with proper care; nerve irritation without structural damage
- Persistent numbness (weeks to months) — Risk of nerve damage increases; requires assessment and intervention
- Chronic numbness (months to years) — May involve permanent nerve changes; restoration of full sensation becomes less predictable
Sign 4: Muscle Weakness in Precise Movement Patterns
Muscle weakness from a bulging disc isn't generalized fatigue. It's specific.
You might have trouble lifting your foot when you walk—that's foot drop, caused by L5 nerve compression affecting the muscles that dorsiflex the ankle. Or you might struggle to push up on your toes—that's calf weakness from S1 compression affecting the gastrocnemius and soleus muscles.
You trip more often. One leg feels heavy. That's not aging—that's an L5 nerve root not firing correctly because a disc is pressing on it. Each nerve root controls specific muscle groups, and when the nerve is compressed, the signal from your brain to those muscles is interrupted. The muscle doesn't fire correctly, and weakness develops.
Some patients notice it as clumsiness. They trip more often. One leg feels "heavy." They have trouble going up stairs or getting out of a chair without using their arms. These aren't signs of aging or deconditioning. They're signs of nerve compression.
Shockwave Therapy can support recovery when muscle weakness has been present long enough to cause compensatory movement patterns, but the primary focus remains on reducing the nerve compression that's causing the weakness in the first place.
The Progressive Nature of Nerve Compression
Weakness often starts subtle. You don't notice it until you try to do something specific—walk on your heels, stand on one leg, push off forcefully when running.
If the compression continues, the weakness becomes more pronounced.
What started as occasional clumsiness turns into consistent difficulty with specific movements.
This is a structural problem that requires structural intervention. Rest won't restore nerve function if the disc is still pressing on the nerve. You need to reduce the mechanical pressure—and that requires identifying which positions, movements, and postural patterns are maintaining the compression.
| Nerve Root | Muscle Groups Affected | Test You Can Do at Home |
|---|---|---|
| L4 | Quadriceps (front of thigh), tibialis anterior (shin) | Try standing from a seated position without using your hands; weakness makes this difficult |
| L5 | Tibialis anterior (foot dorsiflexors), extensor hallucis longus (big toe lifter) | Walk on your heels with toes pointed up; weakness causes foot drop or inability to hold position |
| S1 | Gastrocnemius and soleus (calf muscles), hamstrings | Stand on one leg and push up onto your toes repeatedly; weakness prevents full range or causes early fatigue |
Sign 5: Symptoms That Worsen With Sitting, Bending, or Twisting

Sitting increases pressure on your lumbar discs by up to 40% compared to standing. Bending forward increases it even more.
If you have a bulging disc, these positions push the bulge further into the nerve root. That's why your symptoms flare when you sit for an hour, bend to tie your shoes, or twist to reach something behind you. The Cleveland Clinic Journal of Medicine notes that positional symptom patterns are among the most reliable indicators of disc-related nerve compression.
Standing and walking often provide relief because they reduce disc pressure. The spine is in a more neutral position, the disc isn't being loaded as heavily, and the nerve root has more space.
This positional pattern is diagnostic.
If your pain is mechanical—meaning it gets worse in specific postures and better in others—that's a structural issue. It's not inflammation alone. It's not muscle tightness alone. It's the disc mechanics.
Why "Just Stretch More" Doesn't Fix Positional Pain
Stretching loosens tight muscles. It does nothing to reposition a bulging disc. If the disc is still pressing on the nerve every time you sit, the pain will keep coming back.
If your pain is positional—flaring with sitting, bending, or twisting—you need an approach that addresses the disc mechanics. That means identifying which positions reduce the pressure on the nerve and which increase it, then building a care plan around that information.
Stretching tight hamstrings might give you a few degrees more flexibility. But if the disc is still bulging into the nerve root every time you sit down, the pain will keep coming back.
- Sitting — Increases disc pressure by 40%; worst position for most lumbar disc issues
- Forward bending — Further increases disc pressure; pushes bulge posteriorly into nerve roots
- Twisting while seated — Combines rotational and compressive forces; high-risk movement for nerve compression
- Standing — Reduces disc pressure; often provides immediate symptom relief
- Walking — Promotes blood flow and gentle spinal movement; typically well-tolerated
- Lying supine with knees bent — Minimal disc pressure; often the most comfortable resting position
Why These Signs Keep Coming Back (The Recurrence Problem)

The recurrence problem is simple.
When treatment focuses on calming inflammation or relaxing muscles, symptoms improve temporarily. The anti-inflammatory reduces swelling. The muscle relaxant eases tension. The pain subsides.
But the disc bulge—the structural cause of the nerve compression—hasn't changed.
It's still there. Still pressing on the nerve root. Just with slightly less inflammation around it.
So the next time you sit too long, lift something awkwardly, or twist the wrong way, the nerve gets compressed again. The inflammation returns. The symptoms return. And you're right back where you started.
This is the cycle that defines failed treatment. You get relief, but you don't get resolution. And no one explains why—because most providers are treating the symptom, not the source.
If you want to know whether a herniated disc can heal on its own or if intervention is required, the answer depends on whether the structural pressure on the nerve is being addressed. Spontaneous resolution happens in some cases, but it's not the norm when nerve compression symptoms persist beyond a few weeks.
The Plan Picker Problem
This isn't for someone who wants to pick and choose which parts of the care plan to follow.
If you're told that specific exercises, specific positioning strategies, and spinal adjustments are all necessary to reduce the disc pressure—and you decide to do two out of three—you're going to stay in the cycle.
Partial commitment produces partial results. You'll get some improvement. Then it plateaus. Then the symptoms return. And you'll wonder why the care plan "didn't work."
It didn't work because you didn't follow it.
If that's a problem before we've even started, that's important information for both of us.
What Root-Cause Care Actually Looks Like
Root-cause care for a bulging disc starts with identifying which nerve root is compressed, how severely, and what positions or movements are making it worse.
From there, the care plan is built to reduce the mechanical pressure on that nerve.
That might involve spinal adjustments to restore normal joint motion, specific traction positioning to create space around the nerve root, and movement modification to avoid positions that increase disc pressure.
It's individualized because the location of the bulge, the degree of compression, and your specific triggers are different from the next person's. An L4 bulge with anterior thigh pain requires a different approach than an S1 bulge with calf numbness.
This is also why MRI results might not fully explain what you're experiencing. Imaging shows the anatomy. Clinical assessment shows the function. You need both to build an accurate picture of what's happening and what needs to change.
Frequently Asked Questions
What does a bulging disc in the lower back feel like?
It feels like a deep, persistent ache in your lower back that often radiates down one leg as sharp or burning pain.
You might also experience numbness or tingling in specific areas of your leg or foot—not vague sensations, but precise zones that map to which nerve root is being compressed.
Some people describe muscle weakness in certain movements, like trouble lifting their foot or pushing up on their toes. And most notice that sitting, bending forward, or twisting makes everything worse.
The key marker: these symptoms don't resolve with rest alone. They improve temporarily, then return when you do the activity that increases pressure on the disc.
Can a chiropractor tell if I have a bulging disc without an MRI?
Yes.
A thorough chiropractic assessment—including orthopedic and neurological tests—can identify the tell-tale signs of nerve compression caused by a disc issue.
The pattern of pain (where it radiates), the dermatomal distribution of numbness (which specific zones are affected), the muscle weakness patterns (which movements are impaired), and the positional triggers (which postures make it worse) all provide diagnostic information.
These clinical findings often pinpoint the source of the problem even before imaging is considered. An MRI confirms the anatomical details, but the clinical assessment reveals the functional problem—and that's what determines the care plan.
What is the difference between a bulging disc and a herniated disc?
A bulging disc is when the disc swells and protrudes evenly beyond its normal boundary, like an underinflated tire. The outer layer of the disc (the annulus fibrosus) remains intact.
A herniated disc is when the outer layer cracks, allowing the inner gel-like material (the nucleus pulposus) to leak out. That's a rupture, not just a bulge.
Both can compress nerves and cause similar symptoms, but herniation is typically more severe because the leaked material is highly inflammatory and can cause more intense nerve irritation.
Why do bulging disc symptoms come and go?
Symptoms flare up when an activity or position increases pressure on the affected nerve root. Sitting, bending, twisting—these movements push the disc bulge further into the nerve, triggering pain, numbness, or weakness.
Symptoms may subside with rest because rest reduces the load on the spine and gives inflammation time to calm down. But the structural bulge remains. It's still there, still pressing on the nerve.
So when you return to the activity that increases disc pressure, the nerve gets irritated again and the symptoms return. That's why the cycle repeats. The relief is temporary because the cause hasn't been addressed.
Is walking good for a bulging disc in the lower back?
Gentle walking can be beneficial. It promotes blood flow, reduces spinal pressure compared to sitting, and keeps the surrounding muscles active without overloading the disc.
But it's crucial to listen to your body.
If walking increases your pain, radiating symptoms, or numbness—stop. That's a signal that the current mechanics of your gait or the degree of nerve compression are making things worse, not better.
You should be assessed to understand the specific mechanics of your condition. What works for one person's L5 bulge might aggravate another person's S1 bulge. The answer isn't generic. It's based on your clinical picture.
How long does it take for a bulging disc to heal with chiropractic care?
Timeline depends on several factors: how severe the nerve compression is, how long the symptoms have been present, and how closely you follow the care plan.
Some people see improvement within a few weeks. Others require months of consistent care to reduce the disc pressure and restore normal nerve function.
What's certain: honest timeline assessment happens after the initial evaluation—not before. Anyone who gives you a definitive answer without assessing your specific condition is guessing.
The goal isn't to keep you in care indefinitely. It's to get you to a point where the disc pressure is reduced, the nerve is no longer being compressed, and the symptoms don't return with normal activity.
Can a bulging disc get worse if left untreated?
Yes.
Continued nerve compression can progress from pain to numbness to weakness. If the nerve is compressed long enough, it can sustain structural damage—and that makes recovery harder.
Early intervention focuses on reducing the mechanical pressure before the nerve degenerates. Delayed intervention often means dealing with more extensive nerve damage, longer recovery timelines, and less predictable outcomes.
The longer you wait, the more the nervous system adapts to the dysfunction. And the harder it becomes to restore normal function.
But doesn't the MRI need to show a bulge for it to be real?
No.
Clinical findings—where the pain radiates, which movements trigger it, specific zones of numbness—are often more diagnostically accurate than imaging.
An MRI can show a bulge that isn't causing symptoms. It can also miss the functional nerve compression that is causing symptoms, especially if the compression is positional and the MRI was taken while you were lying flat.
Your body's signals are the data. The pain pattern, the dermatomal numbness, the muscle weakness, the positional triggers—those tell the story. The MRI is one piece of evidence, not the whole picture.
If you're dealing with nerve restoration needs, the assessment starts with what you're experiencing—not with what the imaging shows.
Conclusion
The five signs of a bulging disc in your lower back aren't random. They're your nervous system telling you exactly where the problem is and how severe it's gotten.
Deep pain that won't resolve. Sciatica that follows a nerve pathway. Numbness in specific zones. Muscle weakness in precise patterns. Symptoms that flare with sitting or bending.
These aren't vague complaints. They're diagnostic signals.
And when those signals keep recurring, it's because the structural cause—the disc pressing on the nerve—hasn't been addressed. You've been treating the symptom while leaving the source intact.
That's not bad luck. That's predictable.
If you've been dismissed, told to wait and see, or handed a generic protocol that worked for two weeks and then didn't—this is a different conversation. Unexplained doesn't mean untreatable. It means no one's looked at the right thing yet.
If your lower back symptoms keep cycling between relief and recurrence, that's not a treatment failure on your part. That's what happens when the structural cause stays intact.
A chiropractic assessment at Touch of Wellness Chiropractic starts with what you actually report—where the pain radiates, which movements trigger it, where the numbness shows up. Not a standard protocol. Not a 12-month plan handed over before the evaluation is finished.
If you're in Morton, Peoria, or the surrounding area and want to know what's actually driving your symptoms, find out what your assessment looks like.
Recurring symptoms aren't something you live with. They're something you decode.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet