
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
Why Your MRI Doesn't Show the Real Cause of Your Back Pain
Your doctor pointed to the MRI and said that's the problem. Someone else with the exact same finding has zero pain. That's not an exception—that's the norm. An MRI scan produces a detailed anatomical picture of your spine—bulging discs, herniated discs, spinal stenosis, degenerative changes. But those findings exist in most people who've never had a single day of back pain. That explanation becomes the entire foundation of your treatment plan anyway.
Here's what that explanation doesn't account for: the same structural "abnormalities" your MRI flagged exist in a high percentage of people who have no back pain whatsoever. A systematic review published in the American Journal of Neuroradiology examined MRI findings in asymptomatic populations across all age groups and found disc degeneration, bulges, and protrusions present in people who had never experienced a single day of back pain. Another landmark study in the New England Journal of Medicine reported that 64% of people with no symptoms had at least one abnormal disc finding on their MRI.
Your pain is a functional experience. Your nervous system produces it in response to nerve irritation, muscle imbalances, joint mechanics that have shifted out of normal range, inflammation that an image can't measure. The MRI shows you a snapshot of your anatomy. It does not show you how your body moves, how your nerves are firing, or why your brain is producing a pain signal in the first place. When those two things—what the image shows and what you're actually experiencing—don't line up, the functional picture is what matters. That's what drives the pain. That's what needs to be addressed.
This article breaks down why structural findings on an MRI are often irrelevant to your pain, what a functional assessment actually looks at, and why building a care plan from what you report—not just what a radiologist writes—is the only defensible clinical standard.
Last Updated: April 30, 2026
- Why Structural Findings Don't Always Mean Pain
- What an MRI Actually Shows (And What It Doesn't)
- The Functional Diagnosis You're Not Getting
- Why Treatment Based Only on Imaging Fails
- What to Look for in a Chiropractic Assessment
- FAQ
- Can you have a bulging disc on an MRI and have no pain?
- What causes back pain if my MRI results aren't the reason?
- Should I ignore my MRI results completely then?
- What is a functional chiropractic assessment?
- What happens when a doctor only treats the MRI report?
- How do I know if I need a second opinion on my MRI-based treatment plan?
- If the MRI isn't the answer, what should I be asking my provider?
- Why doesn't my insurance cover functional assessments the same way it covers MRIs?
- Conclusion
Why Structural Findings Don't Always Mean Pain
Your doctor pointed to a bulging disc on your MRI and said that's the problem.
Someone else with the exact same bulging disc—same location, same severity—is walking around with no back pain at all. They don't know the disc is there. They've never felt it. If they got an MRI for an unrelated reason tomorrow, the radiologist would write the same report yours got.
But they're fine.
That's not an exception. That's the norm across the population. The American Journal of Neuroradiology published a systematic review that scanned people who'd never had back pain. Disc degeneration showed up in 37% of 20-year-olds. By age 50, that number was 80%. Disc bulges were present in 30% of people in their twenties. Disc protrusions in 29% of people in their thirties.
Not people who had pain and recovered. People who'd never had back pain in the first place.
The New England Journal of Medicine ran the same test. They scanned 98 people with no symptoms. 64% had at least one abnormal disc finding. More than half. The MRI flagged a "problem," but there was no problem to feel.
The Cookie-Cutter Protocol Problem
Most offices see a bulging disc on an MRI and run the same treatment sequence regardless of what the patient reports.
Walk in with nerve pain, walk in with a headache, walk in with sciatica—you get the same sequence. When it doesn't work, they run it again.
That's not a care plan. That's a template.
The MRI becomes the diagnosis. Your pain history—when it started, what makes it worse, whether it radiates or stays local, how it affects your sleep and your ability to move—gets filtered through the diagnosis code. The code says L4-L5 disc bulge. The protocol says treat the disc. What you actually feel becomes secondary data.
The Cookie-Cutter Protocol assumes the image tells the whole story. It doesn't. The image shows anatomy. It doesn't show nerve function. It doesn't show how your body compensates when one joint stops moving right. It doesn't show inflammation. It doesn't show the muscle guarding pattern you've developed to avoid triggering the pain.
All of that—what's actually driving the signal your brain interprets as pain—is invisible on the scan.
So the provider treats what they can see and ignores what you're reporting. When the treatment doesn't work, they run the same protocol again. When it still doesn't work, they escalate—more injections, stronger medications, surgery.
The problem wasn't that the treatment failed. The problem is they were treating the wrong thing from the beginning.
What the Research Actually Shows
The data on asymptomatic MRI findings isn't new. It's been consistent across multiple studies for decades.
According to the American Journal of Neuroradiology systematic review:
- Disc degeneration prevalence increases steadily with age—37% of 20-year-olds, 52% of 30-year-olds, 68% of 40-year-olds, 80% of 50-year-olds, 88% of 60-year-olds, and 93% of 70-year-olds
- Disc bulges were found in 30% of 20-year-olds, 40% of 30-year-olds, 50% of 40-year-olds, 60% of 50-year-olds, 69% of 60-year-olds, and 77% of 70-year-olds
- Disc protrusions appeared in 29% of people in their twenties, 31% in their thirties, 33% in their forties, 36% in their fifties, 38% in their sixties, and 43% in their seventies
All asymptomatic. None of these people were patients. They had no pain complaints.
The New England Journal of Medicine study reinforced the same pattern. 64% of participants with no back pain had structural findings their MRI flagged as abnormal. Disc bulges, herniations, nerve root compression—all present. All producing zero symptoms.
Your MRI finding isn't rare. It's not an automatic explanation for your pain. And treating it as if it were—without ever asking what your body is actually doing in response—is why so many people go through treatment after treatment and still hurt.
| Age Range | Disc Degeneration (%) | Disc Bulge (%) | Disc Protrusion (%) |
|---|---|---|---|
| 20s | 37 | 30 | 29 |
| 30s | 52 | 40 | 31 |
| 40s | 68 | 50 | 33 |
| 50s | 80 | 60 | 36 |
| 60s | 88 | 69 | 38 |
| 70s | 93 | 77 | 43 |
Data from AJNR systematic review of MRI findings in asymptomatic populations
When the MRI Shows a Problem but You Feel Fine
The inverse scenario happens more often than you'd think.
You get an MRI for something unrelated—a car accident screening, a pre-employment physical that required imaging, a diagnostic workup for another condition. The scan comes back. The radiologist's report lists three bulging discs, mild stenosis, and degenerative changes at L5-S1.
You read that report and suddenly you're worried.
You start paying attention to your back in ways you never did before. You wonder if you should be feeling something. You Google the terms. You read about worst-case outcomes. You start moving more carefully.
And then the pain starts.
Not because the structure changed. The structure was already like that. It's been like that for years. But now you know about it. And that knowledge—combined with the fear the report created—shifts how you move, how you hold tension, how your nervous system interprets normal sensation.
The MRI didn't diagnose a problem. It created one.
This is the danger of imaging without symptoms. The picture becomes a self-fulfilling prophecy. The label produces hyperawareness. Hyperawareness produces guarding. Guarding produces compensatory movement patterns. And those compensations—over weeks or months—can create the very pain the original "abnormality" was never causing in the first place.
If you're moving fine, sleeping fine, functioning fine—an incidental finding on an MRI is just data. It's not a diagnosis. It's not a treatment target. It's information about your anatomy, not a prediction of your future.
What an MRI Actually Shows (And What It Doesn't)
An MRI measures water content in your tissues. That's the mechanism.
Hydrogen atoms in water molecules respond to magnetic fields. The scanner detects those responses and converts them into an image of your anatomy—bones, discs, ligaments, spinal cord, nerve roots.
It's a structural picture. A snapshot. It shows position, size, shape, and hydration status of the tissues the scanner passed through.
What it doesn't show: how those tissues are functioning.
MRI Is a Structural Tool
MRI is exceptional at ruling out serious conditions.
Fractures. Tumors. Infections. Cauda equina syndrome—the medical emergency where nerve compression in the lower spine threatens bowel and bladder control. Spinal cord compression from stenosis severe enough to require surgical decompression.
These are the scenarios where MRI is clinically necessary. It answers a yes-or-no question: is there a structural problem that requires immediate intervention?
For mechanical back pain—the kind that comes from how your body moves, how your joints align, how your muscles compensate—MRI doesn't answer that question. Because mechanical pain isn't a structural diagnosis. It's a functional one.
The National Institute of Neurological Disorders and Stroke states that most low back pain is mechanical or non-organic. Not caused by fracture, tumor, infection, or nerve damage that shows up on imaging. Caused by how the system is working—or not working.
When MRI is used to explain that kind of pain, it's being asked to do something it was never designed for. It can show you a bulging disc. It can't tell you if that disc is the reason you can't sleep, can't sit through a meeting, or can't pick up your kid without your back locking up.
That's not a limitation of the technology. It's a misapplication of it.
What MRI Can't Measure
MRI is a still image. Your pain is a dynamic process.
It can't measure nerve irritation. Nerves don't light up differently on an MRI just because they're firing incorrectly. They don't show inflammation unless there's significant tissue swelling visible in the scan—and by that point, the problem is severe enough that you already know something's wrong.
MRI can't show muscle tension patterns. It can't show joint range of motion restrictions. It can't show how your sacroiliac joint has been compensating for a lumbar restriction for the last six months. It can't show that your hamstrings are constantly guarding because your nervous system is protecting against a movement it perceives as threatening.
It can't show how your brain is processing pain signals.
Your brain produces pain—a decision it makes based on input from nerves, muscles, joints, and past experience. Two people with identical MRI findings can have completely different pain experiences because their nervous systems are responding differently.
That's why you can have a "severe" herniation on your scan and minimal pain, or a "mild" bulge and pain that's debilitating. The severity on the image and the severity of your symptoms are not the same thing.
If your pain is driven by nerve-related conditions like irritation at the nerve root, muscle guarding from chronic tension, or compensatory movement patterns your body developed to avoid triggering the pain—none of that shows up on the scan. This kind of interference with your sleep and participation in activities is a sign that the problem is past the point of waiting it out.
You need a functional test. You need someone to watch you move, test your reflexes, palpate for joint restrictions, and ask what positions make it worse.
That's clinical data. The MRI is supplemental.
| MRI Findings | What It Measures | What It Doesn't Measure |
|---|---|---|
| Bulging Disc | Disc position and hydration level | Whether that bulge is compressing a nerve or causing pain |
| Herniated Disc | Extent of nucleus pulposus protrusion | Nerve irritation, inflammatory response, or functional compensation |
| Spinal Stenosis | Narrowing of the spinal canal | How much space the nerves actually need, or if symptoms correlate with the stenosis |
| Degenerative Changes | Bone spur formation, disc height loss | Joint mobility, muscle compensation, or pain generation |
| Facet Joint Arthritis | Joint space narrowing, bone changes | Range of motion restriction, inflammatory pain, or functional limitation |
The Functional Diagnosis You're Not Getting

A functional diagnosis answers the question the MRI can't: what is your body actually doing?
Not what it looks like. What it's doing.
How far can you rotate your spine before the pain starts? Which specific movement triggers it—flexion, extension, lateral bending, or rotation? Does the pain change when you shift your weight to one leg? Does it radiate when you extend your leg, or does it stay local? What happens when you try to stand from a seated position? Can you bend forward and touch your toes, or does your lumbar spine lock up halfway down?
These are functional questions. The answers come from testing, not imaging.
How a Functional Assessment Works
A chiropractic functional exam evaluates movement, nerve response, and tissue quality in real time.
Range of motion testing identifies mechanical restrictions. If your lumbar spine won't rotate to the left as far as it rotates to the right, that asymmetry is data. It tells you where the joint mechanics have broken down. MRI doesn't measure that. It shows you what the joint looks like at rest. It doesn't show you what happens when you ask it to move.
Orthopedic tests provoke specific tissues to locate the pain generator.
A straight leg raise test loads the sciatic nerve and the hamstring. If it reproduces your pain, that's a positive finding—nerve irritation or hamstring involvement. Kemp's test loads the facet joints on one side by combining extension and rotation. If that reproduces your pain, the facets are involved. Valsalva test increases intrathecal pressure—if your pain spikes when you bear down, that suggests disc involvement.
Each test answers a functional question. And those answers—combined—build the clinical picture.
Neurological testing evaluates how your nervous system is responding. Reflex checks at the knee and ankle tell you if nerve conduction is intact. Sensory testing maps areas of numbness or altered sensation. Motor strength testing identifies weakness patterns that suggest nerve root compression.
Palpation assesses tissue quality and joint motion. A vertebral segment that won't move when you apply pressure—compared to the segments above and below it—is a restriction. Muscle tissue that's hypertonic and won't release under palpation is guarding.
These are mechanical findings. They don't show up on MRI. But they're often the primary drivers of the pain you're experiencing.
This is individualized, root-cause chiropractic care. The assessment is built from what your body does, not from what a radiologist's report says it should do.
Why Your Symptoms Matter More Than the Image
The standard model says the MRI finding is the diagnosis.
A bulging disc at L4-L5 becomes "the problem." The treatment plan is built around that label. What you actually feel—when the pain starts, what positions make it worse, whether it radiates down your leg or stays in your low back, whether it's sharp or dull, constant or intermittent, whether it wakes you up at night or only bothers you after sitting for an hour—all of that becomes secondary information.
That's backwards.
The symptoms are the primary data. The MRI is supplemental.
If your pain doesn't match the expected presentation for an L4-L5 disc bulge—if it's in the wrong distribution, if it's triggered by movements that shouldn't provoke a disc, if you have no neurological deficits but the pain is severe—then the disc isn't the driver. Something else is.
And building a care plan around the disc finding while ignoring what you're reporting is a setup for failure.
Real answers are more valuable than comfortable ones. The comfortable answer is "your MRI shows a bulge, we'll target the bulge." The real answer is "your pain is functional, and we need to figure out what's driving the nerve response—whether that's joint mechanics, muscle compensation, postural stress, or something else entirely."
That second answer requires more work. It requires listening. It requires testing. It requires a provider willing to change the plan if what they're doing isn't producing results.
But it's the only answer that leads to resolution instead of repetition.
The Difference Between Structural and Functional Problems
Most back pain is mechanical.
It's a movement problem. A joint problem. A nervous system overreaction problem. The structure might look "abnormal" on a scan—degenerative changes, disc bulges, facet arthritis—but those findings are common across the population.
What's not common is the functional breakdown that turns a structural variation into a pain-generating problem.
Your spine might have a disc bulge at L4-L5. That's the structure. But the reason that disc is bulging in the first place might be that your L5-S1 joint stopped moving six months ago and L4-L5 has been compensating ever since. The bulge is the effect. The L5-S1 restriction is the cause.
Treating the effect—injecting the bulge, surgically trimming the bulge—doesn't fix the cause. So the compensatory load continues. And the pain either doesn't resolve or it shifts to a different area because the functional problem is still there.
The function is what broke. The structure is just showing you the damage.
| Structural Issue (MRI Finding) | Functional Issue (Underlying Cause) | Why It Matters |
|---|---|---|
| Herniated Disc | Nerve compression from joint misalignment or loss of normal spinal curve | The disc may not be the pain generator—the misalignment created the herniation and continues to irritate the nerve |
| Spinal Stenosis | Reduced range of motion causing nerve impingement during specific movements | The stenosis may be present but asymptomatic until movement dysfunction triggers nerve compression |
| Degenerative Disc Disease | Loss of shock absorption due to chronic postural stress or repetitive loading patterns | The degeneration is the result of mechanical stress—treating the disc without correcting the load pattern doesn't stop progression |
| Facet Joint Arthritis | Muscle guarding and compensatory movement limiting joint mobility | The arthritis is visible but the functional restriction and muscle tension are what produce the pain signal |
| Spondylolisthesis (vertebral slippage) | Core weakness or pelvic instability allowing excessive vertebral motion | The slip is structural but may be stable—pain comes from the unstable movement pattern, not the slip itself |
Why Treatment Based Only on Imaging Fails

When the treatment plan is built from the MRI report alone—ignoring what the patient reports, ignoring how they move, ignoring what functional tests reveal—outcomes are poor.
Patients get epidural steroid injections targeting a disc bulge. The pain improves for two weeks. Then it comes back.
Doctor says the injection didn't work. Next step: surgery.
But the injection targeted the structure. It reduced inflammation around the disc. It never addressed why the nerve was irritated in the first place. The joint restriction that created the compensatory load on that disc? Still there. The muscle guarding pattern? Still there. The postural dysfunction? Still there.
So the functional problem continues. And the pain returns.
This is what happens when you treat the symptom and leave the cause alone.
The Insurance-Reimbursement Trap
The current reimbursement model incentivizes volume and procedure codes, not outcomes.
An MRI-based diagnosis code justifies billing. L4-L5 disc bulge with radiculopathy—that's a code. Insurance pays for the injection. Insurance pays for the follow-up. If the injection doesn't work, insurance pays for surgery.
A functional assessment that concludes "your L4 disc bulge isn't the problem, your sacroiliac joint mechanics are, and we need to address the SI joint restriction and the compensatory muscle patterns you've developed" doesn't fit neatly into that system.
There's no procedure code for "spent 45 minutes evaluating joint mechanics, palpating for restrictions, testing nerve function, and mapping pain provocation patterns." There's a code for a chiropractic adjustment, but the critical assessment work that determines if it's the right intervention isn't separately reimbursed. It's bundled into the visit.
So the structural diagnosis wins by default. Not because it's more accurate. Not because it produces better outcomes. Because it's easier to bill.
This is a system problem, not a clinical one. But patients pay the price. They get treatments aimed at anatomical findings while the functional drivers of their pain are never addressed. And when the treatment doesn't work, they're told they need more of the same—or something more invasive.
That's not care. That's a revenue cycle.
When the "Fix" Doesn't Fix Anything
You got an epidural steroid injection. Your pain dropped from an 8 to a 3 for about two weeks. Then it climbed back to a 7.
Your doctor says the injection didn't hold. Time to consider surgery.
Here's what actually happened: the injection reduced inflammation around the disc. Inflammation is one component of nerve irritation. But it's not the only component. The mechanical load on that disc—the reason it was inflamed in the first place—never changed. The joint above it that stopped moving and forced the disc below to compensate? Still restricted. The muscle guarding pattern you developed to avoid the pain? Still firing.
So the inflammation came back. Because the cause is still there.
The injection worked exactly as designed. It reduced inflammation. But inflammation was the symptom. The cause was mechanical. And mechanical problems don't resolve with a chemical intervention.
This is where patients get stuck in loops. Injection doesn't work. Try a different injection. Still doesn't work. Try physical therapy—but the PT protocol is generic, built around the diagnosis code, not around your specific functional breakdown. Doesn't work. Back to the doctor. MRI still shows the bulge. Surgery is the next step.
But surgery targets the bulge. It trims the disc material, decompresses the nerve, maybe fuses the segment if the instability is severe enough. What it doesn't do: restore normal joint mechanics to the segments above and below. Retrain the muscle patterns. Address the postural dysfunction that created the compensatory load in the first place.
So the pain might improve short-term. Long-term? It often shifts. Adjacent segment degeneration is common after spinal fusion because the segments next to the fusion now have to handle the load the fused segment used to carry. And if the functional cause—the thing that started the whole cascade—was never addressed, those adjacent segments break down faster.
This is the cycle. Treat the structure. Ignore the function. Repeat when it doesn't work. Escalate when repetition fails.
If you've been stuck in that cycle—if you're dealing with chronic or recurring pain that temporarily improves and then returns—the problem isn't that the treatments are bad. The problem is they're aimed at the wrong target.
What Happens When You Change Course
If a treatment isn't working and you keep doing it anyway, that's the clinical definition of failure.
The willingness to stop, reassess, and pivot when something isn't producing results is the marker of a competent provider.
Care plans that adapt based on patient response—not based on what the initial MRI showed—produce better outcomes. Because they're built on reality, not assumptions.
If the first approach doesn't reduce your pain or restore your function after a reasonable trial period, a competent provider doesn't repeat it. They reassess. They ask what changed, what didn't change, and what that tells them about the functional drivers they might have missed.
Maybe the initial hypothesis was wrong. Maybe the primary restriction isn't where they thought it was. Maybe there's a compensatory pattern further up or down the chain that needs to be addressed first. Maybe the nervous system response is more protective than they initially assessed, and the treatment intensity needs to be adjusted.
All of that requires a provider who's willing to listen, test, and change course.
The alternative is running the same protocol and hoping it works this time. That's not clinical judgment. That's stubbornness.
Patients who get better—patients who go from constant pain to functional—aren't the ones who got lucky with the first treatment. They're the ones whose provider was willing to adjust the plan when the first approach didn't produce the expected result.
That adaptability is what separates individualized care from assembly-line protocols. And it's the reason some patients resolve in a few weeks while others spend years cycling through the same failed treatments.
What to Look for in a Chiropractic Assessment
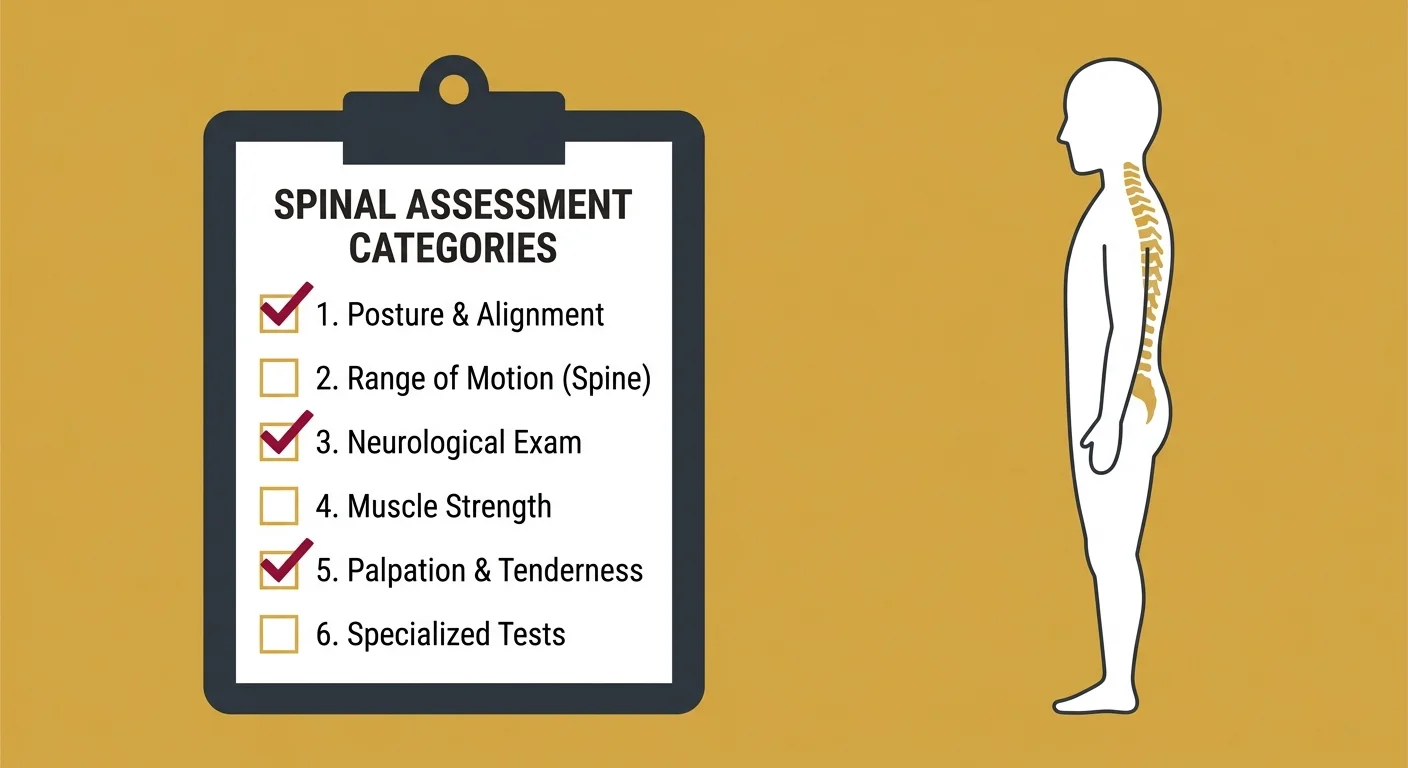
If you're looking for a provider who's going to do more than glance at your MRI and hand you a generic care plan, here's what the first visit should include.
Not as a checklist to memorize. As a baseline for what functional assessment actually looks like.
Range of Motion and Orthopedic Testing
Range of motion testing identifies mechanical restrictions.
Your provider should be watching you move—forward flexion, extension, lateral bending to each side, rotation to each side. They're not just checking if you can do the movement. They're checking how far you can go, whether the movement is symmetrical, and whether it reproduces your pain.
If you can rotate 45 degrees to the right but only 30 degrees to the left, that asymmetry is data. It tells you where the restriction is. If forward flexion stops halfway down and you feel a pulling sensation on one side, that tells you where the tissue is guarding.
Orthopedic tests provoke specific structures to locate the pain generator.
Straight leg raise loads the sciatic nerve and the hamstring. If lifting your leg while lying flat reproduces your leg pain, that's nerve involvement. Kemp's test combines extension and rotation to load the facet joints. If that reproduces your back pain, the facets are part of the problem. Patrick's test (FABER test) assesses the hip and sacroiliac joint. Valsalva increases pressure inside the spinal canal—if bearing down makes your pain worse, that suggests disc involvement.
Each test is a question. The answer—positive or negative, pain or no pain—builds the picture of what's actually happening in your body.
These are functional assessments. They show how your body moves under load. MRI shows how it looks at rest. The difference matters.
Neurological and Palpation Findings
Reflex testing checks nerve conduction.
Your provider taps your patellar tendon at the knee. Your quadriceps should contract and your leg should kick slightly. That's an L4 nerve root reflex. They tap your Achilles tendon. Your calf should contract. That's an S1 reflex. If the reflex is absent or diminished on one side, that's a sign of nerve root compromise.
Sensory testing maps areas of altered sensation. They run a pinwheel or their fingers along your leg. You report where it feels normal, where it feels dull, where it feels sharp. Specific dermatome patterns correspond to specific nerve roots. If you've lost sensation in a strip down the outside of your calf, that's L5. Inner thigh? L2-L3.
Motor strength testing identifies weakness. They ask you to push against resistance—dorsiflexion (pull your toes toward your shin), plantarflexion (push down like you're stepping on a gas pedal), hip flexion, knee extension. If one side is noticeably weaker than the other, that's motor involvement from nerve compromise.
Palpation assesses joint motion and tissue quality in real time.
Your provider applies pressure to each vertebral segment and feels for movement. A segment that moves normally when pressed will spring back slightly. A segment that doesn't move—compared to the ones above and below it—is restricted. That restriction is a mechanical problem. It doesn't show up on MRI. But it's often the primary driver of compensatory pain.
Muscle palpation identifies guarding. If a muscle is hypertonic—tight, ropy, won't release under sustained pressure—that's your nervous system protecting against a perceived threat. The muscle isn't the problem. It's responding to something else. But that guarding pattern contributes to the pain cycle and needs to be addressed.
These findings—reflexes, sensation, motor strength, joint motion, tissue quality—are the functional data your MRI can't provide. And when they don't line up with the MRI findings, the functional data is what drives the care plan.
Building the Care Plan From What You Report
Individualized care is not optional. It's the clinical standard.
A care plan built from what you actually report—your pain triggers, your movement limitations, your daily function gaps, how your symptoms change based on position or activity—will always be more accurate than one built from a radiologist's written impression of your L4-L5 disc.
The MRI is one data point. Your history is another. The orthopedic and neurological findings are another. Palpation findings are another. When you combine all of those, you get a clinical picture. And that picture determines the treatment approach.
If your MRI shows a bulge but your orthopedic tests are negative, your reflexes are intact, and your pain is reproduced by SI joint provocation, the bulge isn't the target. The SI joint is. Treat the SI joint restriction, address the muscle compensation, and the pain resolves—even though the MRI still shows the bulge.
That's what happens when the care plan is built from function instead of imaging.
If you're looking for the primary signs of a bulging disc and your symptoms don't match, that's valuable information. It tells you the bulge might not be the driver. And a provider who listens to that—who adjusts the plan based on what you're experiencing—is doing their job correctly.
FAQ
Can you have a bulging disc on an MRI and have no pain?
Yes. It's very common.
Research from the American Journal of Neuroradiology shows that disc bulges are present in 30% of people in their twenties, 40% in their thirties, 50% in their forties, and higher percentages as age increases. These are people with no back pain. They didn't know the bulge was there. They've never felt it.
The presence of a bulge on an MRI doesn't predict pain. Plenty of people have structural "abnormalities" and zero symptoms. The bulge becomes a problem only when it creates functional issues—nerve compression, inflammation, or movement restrictions that produce a pain signal.
If your MRI shows a bulge but your pain doesn't match the expected pattern for that finding, the bulge probably isn't the cause.
What causes back pain if my MRI results aren't the reason?
Back pain is often functional.
Nerve irritation from joint misalignment. Muscle imbalances creating compensatory load. Postural stress from repetitive movement patterns. Inflammation that an MRI can't measure unless it's severe enough to show tissue swelling. Guarding patterns where your nervous system restricts movement to protect against a perceived threat.
The body's response to an issue is often what creates the pain signal, not the anatomical structure the MRI flagged.
A disc bulge might be present, but if your sacroiliac joint stopped moving six months ago and your lumbar spine has been compensating ever since, the SI joint restriction is the functional cause. The disc bulge is the effect. Treating the disc without addressing the SI joint doesn't resolve the problem.
That's why functional assessment matters. It identifies what your body is actually doing—not just what it looks like.
Should I ignore my MRI results completely then?
No. MRI is a valuable tool for ruling out serious conditions.
Fractures. Tumors. Infections. Cauda equina syndrome. Severe spinal stenosis requiring surgical decompression. These are the scenarios where MRI is clinically necessary. If your MRI rules those out, that's important information.
But once serious pathology is off the table, the MRI findings should be one piece of a larger clinical picture—not the sole driver of your care plan.
If your MRI shows a bulge but your functional assessment shows the pain is coming from a different source, the functional data is what you treat. The MRI told you what's there. The functional assessment told you what's causing the pain.
Context from functional assessment and symptom reporting is required to make the MRI findings clinically meaningful.
What is a functional chiropractic assessment?
A functional assessment evaluates how your body actually performs.
Range of motion testing. Orthopedic provocation tests. Neurological reflex and sensory checks. Palpation for joint restrictions and muscle guarding. Pain mapping—what positions trigger it, what positions relieve it, whether it radiates or stays local.
It's not a static picture. It's a dynamic evaluation of how you move, where your restrictions are, and how your nervous system is responding.
The goal is to identify the functional drivers of your pain—the things an MRI can't show. Joint mechanics. Muscle compensation. Nerve irritation. Postural dysfunction. These are the variables that determine whether a structural finding becomes a pain-generating problem or stays asymptomatic.
A functional assessment provides the context the MRI lacks.
What happens when a doctor only treats the MRI report?
Treatment targets the structural finding without addressing the functional cause.
You get an injection aimed at the disc bulge. The pain improves temporarily because the inflammation around the disc is reduced. But the joint restriction that created the compensatory load on that disc is still there. The muscle guarding pattern is still there. The postural dysfunction is still there.
So the inflammation comes back. And the pain returns.
When the treatment is based only on imaging, it misses the functional breakdown that's driving the pain. Patients end up in cycles—repeated injections that don't hold, physical therapy protocols that don't address the root restriction, surgeries that reduce one problem but create adjacent segment issues because the functional cause was never corrected.
If your primary care physician recommends surgery based solely on your MRI and hasn't done a functional assessment, that's a red flag. Surgery might be necessary. But it shouldn't be the first answer when the functional picture hasn't been evaluated.
How do I know if I need a second opinion on my MRI-based treatment plan?
If your symptoms don't match the expected pattern for the MRI finding, that's a signal.
Your MRI shows a herniated disc at L4-L5. But your pain is in your hip, not down your leg. Or your pain is worse with extension, not flexion—which is the opposite of what a disc herniation typically produces. Or you have no neurological deficits—no numbness, no weakness, no reflex changes—but the pain is severe.
When the clinical presentation doesn't align with the imaging findings, the imaging might not be showing the primary problem.
Ask your provider: "If my symptoms changed tomorrow, would the treatment plan change?" If the answer is "no, we treat the MRI regardless," that's a problem. The care plan should be driven by what you're experiencing, not by a static image.
The disc might be severe structurally. But if your symptoms don't match, the disc might not be the driver. Severity on the scan and severity of symptoms are not the same thing.
If the MRI isn't the answer, what should I be asking my provider?
Ask what functional tests were done.
"What did the range of motion testing show? What did the orthopedic tests reveal? What are my reflex and sensory findings? Where did you palpate restrictions?"
If the answer is "we didn't do those tests, we're going off the MRI," that's incomplete assessment.
Ask how your symptoms align with the MRI findings.
"My pain is in my hip and outer thigh, but the MRI shows a disc bulge at L4-L5. Does that distribution match what you'd expect from an L4-L5 problem?"
If the answer is vague or dismissive, push for clarity.
Ask if the care plan would change if your symptoms changed.
"If my pain moved to a different area or got worse with different movements, would you reassess and adjust the treatment, or would you keep following the MRI-based plan?"
If the answer is "we'd keep following the plan," that's a protocol, not individualized care.
You deserve a provider who builds the care plan from what you report, not from what a radiologist wrote in a report.
Why doesn't my insurance cover functional assessments the same way it covers MRIs?
Insurance reimbursement is built around diagnosis codes and procedures, not outcomes.
An MRI has a billing code. It's a discrete service with a defined cost. A provider orders it. A radiology center performs it. The insurance company pays.
A functional assessment—45 minutes of range of motion testing, orthopedic provocation, neurological checks, palpation, and pain mapping—doesn't have a separate procedure code. It's bundled into the office visit. The time, the clinical judgment, the manual testing—none of that is separately reimbursed.
So providers who rely on insurance reimbursement are incentivized to order the MRI and build the treatment plan from the imaging. It's faster. It fits the billing model. And it produces a diagnosis code that justifies further procedures.
Functional assessment takes more time. It requires skill. And it doesn't generate billable codes the way imaging and injections do.
This is a system problem. The reimbursement structure doesn't reward the work that actually identifies the cause. It rewards the work that fits into a code.
Patients end up paying the price—not in dollars necessarily, but in outcomes. They get imaging-based care when they needed function-based care. And when the treatment doesn't work, they're told they need more of the same.
That's not care. It's a workflow optimized for billing, not for recovery.
Conclusion
Your MRI shows a structural finding. That finding might be relevant. It might not be.
The only way to know is to look at the functional picture. How do you move? Where are the restrictions? What reproduces your pain? What relieves it? Do your symptoms match the expected presentation for the MRI finding, or are they pointing somewhere else?
Those questions don't get answered by looking at a scan. They get answered by testing, palpating, and listening to what you report.
The nervous system runs everything. When it's disrupted—whether by joint restriction, muscle compensation, postural dysfunction, or nerve irritation—nothing works right. And that disruption doesn't always show up on an image. Sometimes the structure looks fine and the function is broken. Sometimes the structure looks broken and the function is fine.
What you don't need is another provider who builds your entire care plan from a radiologist's report and never asks what you're actually experiencing.
Your care plan is built from what you actually report—not from what a diagnosis code says you should have. If something isn't working after a few visits, we change it. Not repeat it. The willingness to stop and reassess isn't a weakness. It's the whole point.
If your MRI findings and your pain don't line up, that's not a mystery. It's a signal that the assessment stopped too early. Someone looked at the image and called it done. They didn't look at you.
Unexplained doesn't mean untreatable. Dismissed doesn't mean imaginary. It means no one's looked at the right thing yet.
If your MRI pointed to a problem but the treatment didn't work—or if your symptoms don't match what the scan shows—that gap is worth investigating.
An assessment at Touch of Wellness Chiropractic starts with what you report. Not with what the MRI says you should be experiencing. If your pain doesn't fit the structural diagnosis, that's not ignored. That's the starting point.
See what a functional chiropractic evaluation looks like when the care plan is built from how your body actually moves—not from a radiologist's impression of a single frame.
If the image and the pain don't line up, the pain is what needs to be explained. Not explained away. Explained.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet