
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
Your Disc Recovery Plan Is Finished. Now What? How To Maintain Long-Term Spinal Health.
Maintaining disc health after completing a recovery plan requires three non-negotiable components: consistent targeted exercise to stabilize the spinal structures, diligent practice of spinal hygiene in all daily activities, and periodic professional assessment to catch and correct minor biomechanical dysfunction before it escalates into a clinical problem.
The transition from active treatment to maintenance is not passive. Recovery restored function. Maintenance protects it. The distinction matters because most disc re-injuries occur not during the healing phase when patients are cautious and attentive, but months later when old movement patterns and postural habits quietly return. The nervous system adapts to poor mechanics over time, which means you can feel fine while gradually loading your discs in ways that will eventually produce the exact problem you just resolved.
Targeted exercise in this context does not mean general fitness or cardiovascular conditioning. It means specific movements that activate the deep stabilizing muscles of the core and posterior chain—the transverse abdominis, multifidi, and gluteal complex—which provide the structural support your spine requires to handle load safely. These muscles do not strengthen incidentally through walking or yoga. They require intentional, progressive activation patterns that must be practiced consistently to remain effective.
Spinal hygiene refers to the biomechanical awareness required to move through daily tasks without compromising disc integrity. Lifting a laundry basket, sitting at a desk, bending to tie shoes—these are the moments where re-injury occurs, not during dramatic events. Poor lifting mechanics, prolonged static flexion, and repetitive end-range spinal movements place disproportionate stress on the posterior disc where herniation is most likely. Changing these patterns requires conscious reprogramming of habitual movement, which is why maintenance plans emphasize behavioral modification as much as physical conditioning.
Periodic professional check-ups serve a diagnostic function, not a treatment function. They identify asymmetries, compensatory patterns, and early warning signs of biomechanical stress before they produce pain. This is fundamentally different from ongoing treatment for an active problem. The goal is not to keep you coming back indefinitely. The goal is to give you the tools to manage your own spinal health while using professional assessment as a quality control checkpoint—similar to preventive dental care, not ongoing dental surgery.
Last Updated: 2026-04-30
Why Most Disc Injuries Return Within 12 Months

You think recovery means you're done.
That's what breaks it again.
The pain went away. You're moving fine. So everything goes back to normal—same habits, same posture, same workouts. And for six months, nine months, it feels good.
Then you bend wrong. Or sit too long. And the pain's back. Sharp. Radiating. Exactly like before.
That's not an accident. That's the pattern.
The Recovery-to-Relapse Timeline
Here's what nobody tells you when they release you from care.
The urgency fades fast.
Patient finishes recovery. Disc healed. Pain gone. They're released with maintenance instructions—exercises, posture fixes, check-ups.
And for a while, they follow it.
Then the fear goes away. Exercises get skipped. Form gets sloppy. Old habits creep back in.
Six to nine months later, a "random" twinge becomes a full relapse. Same disc. Same symptoms. Sometimes worse.
That's not a recovery failure. That's a maintenance failure.
According to the National Institute of Neurological Disorders and Stroke, ongoing exercise and maintaining a healthy weight are critical for preventing low back pain recurrence. The data's clear—recovery without maintenance gives you temporary results.
What Actually Causes the Re-Injury
The disc healed. The movement patterns didn't.
The postural habits didn't. The muscle imbalances didn't. All the things that broke it the first time? Still there.
Recovery fixed the symptom. Maintenance fixes the cause.
Without maintenance, you're running the same program that broke down before. Your nervous system defaults to what it learned over decades—forward head, weak glutes, poor core activation. That feels normal. Because it is normal for you.
Normal and healthy aren't the same thing.
That's why individualized chiropractic care doesn't stop when pain stops. The plan shifts from corrective to preventive. The goal becomes protecting what you built—not rebuilding what broke.
Pain-Free Months Don't Mean You're Safe
Pain shows up late.
By the time you feel it, the damage is already underway. Months of bad lifting, prolonged sitting, weak core—they don't hurt. Until they do.
Your disc doesn't warn you when it's being loaded wrong. It sends pain when the load exceeds capacity. By then, you're not preventing. You're treating.
That's why maintenance is built on behavior, not pain response. You don't wait for something to hurt before you protect it.
You protect it because you understand what breaks it.
The Three Pillars of Post-Recovery Spinal Health
These three aren't optional.
Remove one, and the whole thing weakens. Partial commitment produces partial results. That's not a threat. That's mechanics.
Pillar 1: Targeted Core Stabilization
Core stability isn't the same as core strength.
Stability means deep spinal stabilizers activate reflexively to hold neutral spine under load. That requires specific motor patterning general ab exercises don't teach.
You can have visible abs and zero functional core stability.
Sit-ups and crunches strengthen the rectus abdominis—the six-pack muscle. They do nothing for the transverse abdominis, multifidi, or pelvic floor. Those are the muscles that actually protect your discs.
Harvard Health emphasizes that core muscles are foundational to spinal support, and strengthening them is primary for long-term back health. But strengthening the right muscles, the right way, is what produces results.
- Transverse Abdominis — Deep corset muscle that creates intra-abdominal pressure and stabilizes spine before movement
- Multifidi — Small muscles along each vertebra controlling segmental motion and preventing shear forces
- Gluteal Complex — Primary hip extensors counterbalancing forward spinal load during lifting and walking
- Pelvic Floor — Foundation of core stability working with diaphragm and transverse abdominis
Pillar 2: Spinal Hygiene in Daily Movement
Every bend, lift, sit, or twist—you're either reinforcing good mechanics or accelerating breakdown.
Spinal hygiene is protecting your discs during the thousand small movements you make every day. It's not restriction. It's precision.
Most disc injuries don't happen during heavy deadlifts. They happen picking up laundry, reaching into your car, tying shoes standing up. That's where your body defaults to habit—and if that habit's flawed, your discs pay.
The Mayfield Clinic outlines proper lifting and posture as core components of disc injury prevention—not recommendations. Requirements. Your spine doesn't respond to intentions. It responds to load.
Pillar 3: Periodic Professional Assessment
Maintenance care isn't ongoing treatment. It's diagnostic.
Assessment identifies compensatory patterns and early dysfunction before symptoms show up. That's catching a problem at stage one instead of stage ten.
Most patients don't notice when they favor one leg, hike a shoulder, or shift weight to avoid loading a segment. Those feel like adaptations. They're creating new stress patterns that'll eventually break down.
That's what a maintenance visit catches. Not an active injury. An active compensation.
"Does maintenance mean I have to keep coming back forever?"
No.
The goal's independence. Periodic check-ups are proactive assessment—like dental cleaning for your spine. Not treatment of an active problem. If you need ongoing treatment, you're not in maintenance. You're back in recovery.
Core Stabilization Exercises That Actually Work
Not all core exercises protect discs.
Some strengthen muscles while destabilizing spine. The exercises that protect are specific, intentional, and different from what most people do.
Transverse Abdominis Activation: The Foundation
The transverse abdominis is your deepest core muscle. Wraps around your midsection like a corset. Creates intra-abdominal pressure that stabilizes spine.
Most people have never consciously activated it.
When you brace properly, your midsection tightens and expands slightly out—not in. You feel pressure building inside your abdomen, like you're about to take a punch. That pressure creates a rigid cylinder around your spine preventing shear and compression from reaching discs.
Learning to brace before lifting or moving is the single most important pattern for disc protection.
Every other exercise builds on this.
Glute Bridges: Posterior Chain Strength
Glutes and hamstrings counterbalance forward spinal load.
Weak glutes force low back to compensate during lifting and walking. Over time, that overloads lumbar discs. Glute bridges rebuild that strength without placing shear stress on discs.
Lie on your back, knees bent, feet flat. Press through heels and lift hips until your body forms a straight line shoulders to knees. Squeeze glutes at top. Lower with control.
That's it. Simple. Foundational. Non-negotiable.
| Exercise Name | What It Strengthens | Why It Matters for Disc Health |
|---|---|---|
| Dead Bug | Transverse abdominis, hip flexors, shoulder stability | Teaches core bracing while moving limbs independently—exact pattern needed for walking and functional movement without spinal compensation |
| Bird Dog | Multifidi, glutes, contralateral core stabilizers | Builds reflexive stabilization and trains nervous system to maintain neutral spine during asymmetrical loading |
| Glute Bridge | Glutes, hamstrings, posterior chain | Counterbalances forward spinal load and prevents low back compensation during lifting and gait |
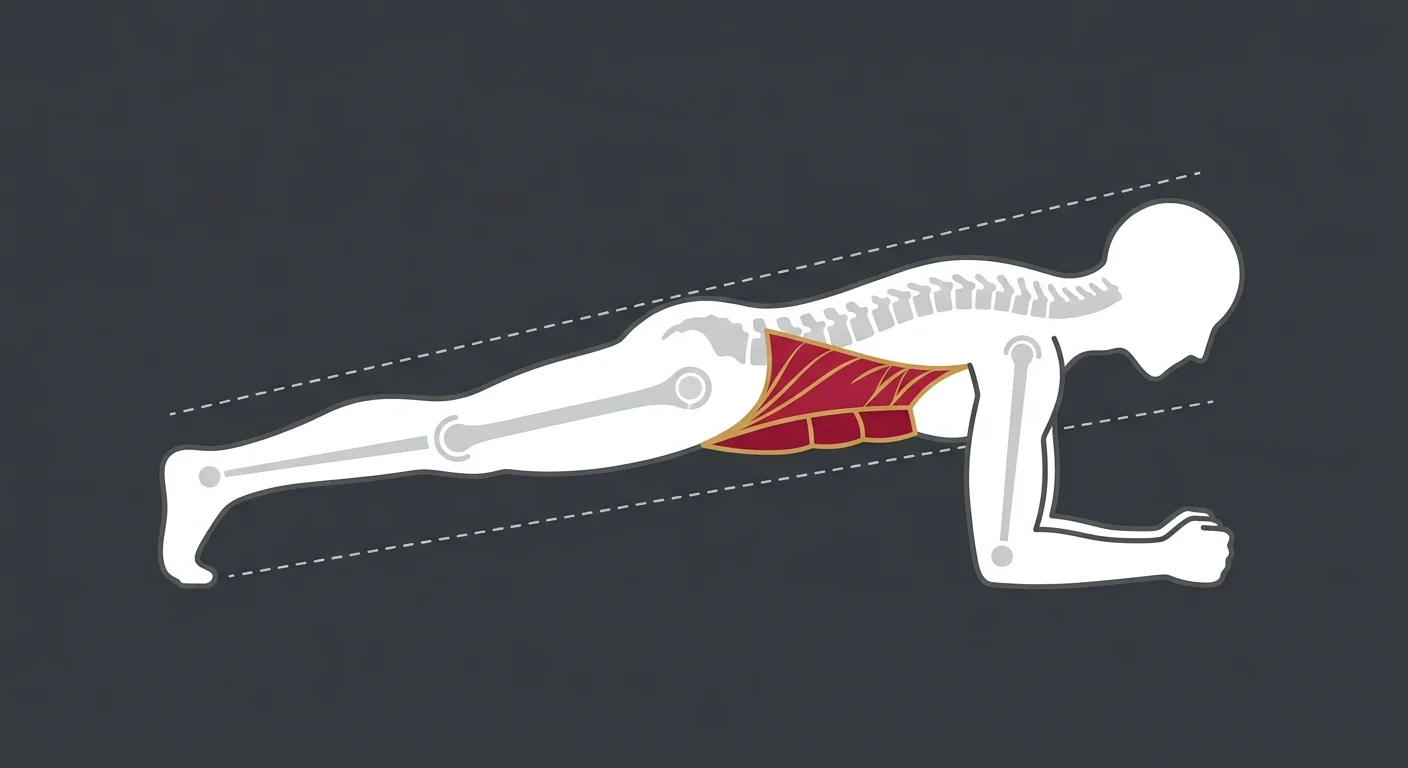
| Plank (proper form) | Transverse abdominis, shoulder girdle, anterior chain | Develops isometric core endurance—but only with neutral spine and active glute engagement (sagging hips = disc stress) |
The Bird Dog: Stability Without Flexion
Bird dog teaches contralateral stability—maintaining neutral spine while moving opposite limbs.
That's the exact motor pattern for walking, running, functional movement. Strengthens stabilizers without spinal flexion. Safe for post-disc-injury patients.
Start on hands and knees. Brace core. Extend right arm forward and left leg back simultaneously. Hold 3-5 seconds. Return. Repeat opposite side.
Goal's not speed. It's control.
If your hips rotate or back arches, you've lost stability. Scale back range and rebuild the pattern correctly.
Research published in The BMJ supports exercise as a key component in both treatment and long-term management of low back pain. But the type of exercise matters as much as consistency.
What NOT to Do: Exercises That Load Discs Dangerously
Sit-ups, crunches, and unsupported forward flexion place extreme compressive and shear forces on lumbar discs.
Standard gym fare. Worst possible choice for disc injury history.
Every sit-up loads your discs with 730 pounds of compressive force at L5-S1. That's measured data. In a flexed position—exact position where discs are most vulnerable to posterior herniation.
If you've had a disc injury, sit-ups aren't core strengthening. They're disc destruction.
Period.
Spinal Hygiene: The Habits That Protect Your Discs
Spinal hygiene isn't one action. It's comprehensive protection during every activity.
These aren't restrictions. They're how you protect what you just rebuilt.
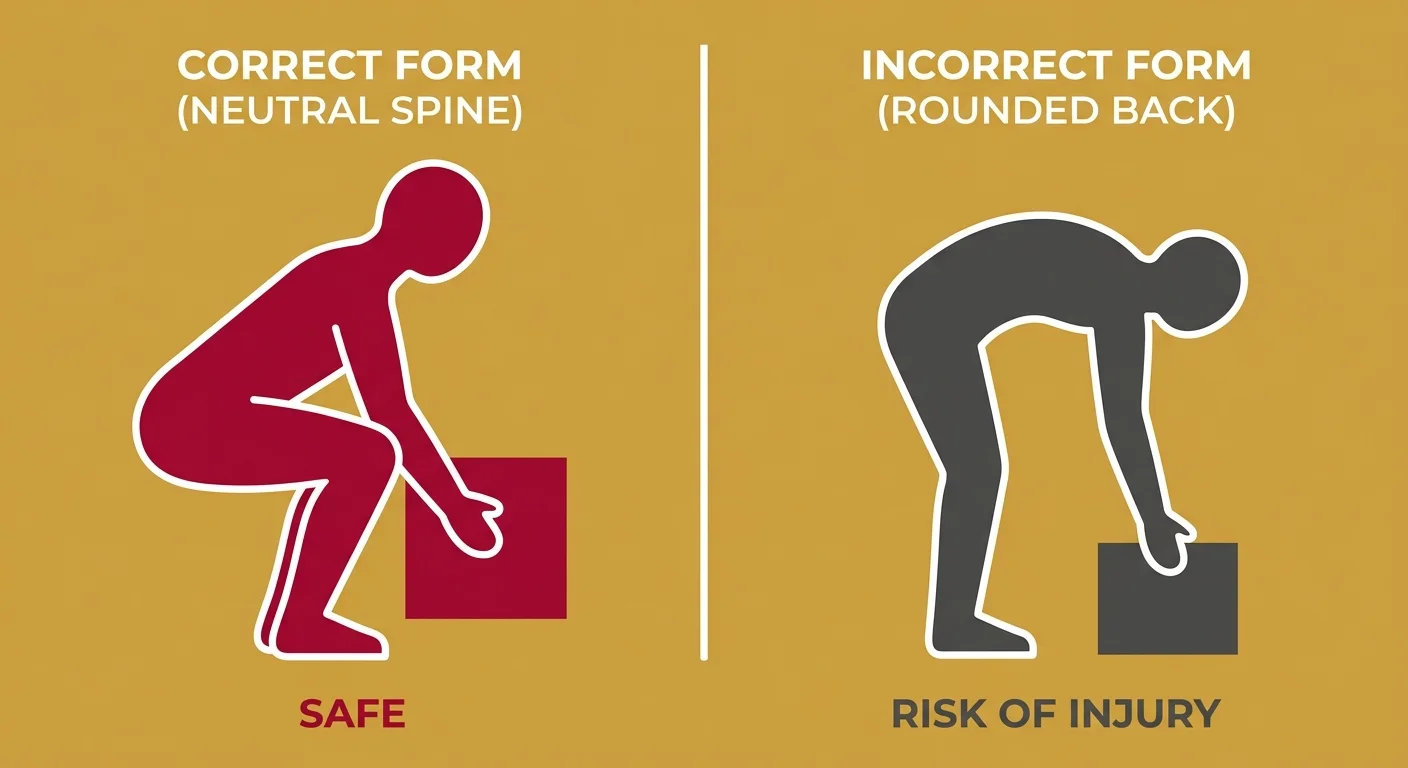
Lifting Mechanics: Hip Hinge, Not Spine Flexion
Every time you pick something up—grocery bag, child, box—your spine's either protected neutral or vulnerable flexed.
Hip hinge protects discs by loading hips and glutes instead of low back.
Here's the difference:
Spine flexion: You bend from waist. Low back rounds. Weight pulls upper body forward. Lumbar discs compress anteriorly and bulge posteriorly—exactly where herniation occurs.
Hip hinge: You push hips back. Spine stays neutral. Glutes and hamstrings load. Weight stays close to center. Discs remain evenly loaded.
One protects. One destroys.
If you're not sure which you're using, film yourself picking something up. If low back rounds, you're flexing. If hips move back and chest stays up, you're hinging.
Understanding sleeping positions for disc recovery is the same principle—neutral spine positioning reduces disc load during vulnerable states.
Sitting Posture: The Static Load Problem
Prolonged sitting in flexed posture places consistent posterior load on lumbar discs.
That's why office workers and drivers have disproportionately high disc injury rates. Not the sitting. The static flexed position held for hours without relief.
Solution isn't better chairs. It's movement breaks, lumbar support, and postural resets every 20-30 minutes.
OSHA provides detailed guidelines for proper workstation setup to minimize spinal load during sedentary work. The guidelines exist because the injury pattern's consistent and predictable.
- Lumbar Support — Small roll or cushion at belt line maintains natural lumbar curve and prevents posterior disc load
- Monitor Height — Screen at eye level prevents forward head posture and cervical strain
- Feet Flat — Feet supported on floor or footrest prevents posterior pelvic tilt
- Movement Breaks — Stand, walk, or reset posture every 20-30 minutes to redistribute disc pressure
If you're the type who picks which maintenance activities to follow based on convenience, this won't work.
Partial commitment produces partial results. Spinal hygiene's all or nothing.
The Morning Routine: Disc Hydration and Flexibility
Discs lose fluid overnight from compressive forces during sleep. Morning's when they're most vulnerable.
When you wake up, discs are maximally hydrated and slightly swollen. That makes them stiffer and less able to handle compression and shear. Bending forward right after waking—tying shoes, picking something up, stretching—places disproportionate stress on discs that aren't ready.
First 30 minutes after waking should include gentle spinal extension, hip mobility, and gradual loading before heavy lifting or bending.
- Cat-cow stretches to restore segmental motion
- Glute bridges to activate posterior chain
- Gentle walking to distribute fluid and warm tissues
- Avoid forward flexion until discs decompress
| Activity | What to Do | Why It Matters |
|---|---|---|
| Lifting objects | Hip hinge with neutral spine, load close to body | Keeps disc pressure even—prevents posterior bulge under load |
| Prolonged sitting | Lumbar support, movement breaks every 20-30 minutes | Static flexion loads posterior disc continuously—breaks redistribute pressure |
| Morning routine | Gentle extension, no forward bending for 30 minutes | Discs are maximally hydrated and vulnerable in morning—gradual loading prevents injury |
| Driving | Lumbar roll, adjust seat to reduce hip flexion | Hip flexion + vibration = posterior disc stress—support and positioning reduce load |
| Bending forward | Hip hinge, not spine flexion | Spine flexion compresses anterior disc and bulges posterior—hip hinge avoids this |
| Twisting movements | Pivot feet, not spine | Rotation + flexion is highest-risk movement pattern for disc herniation |
Twisting Under Load: The Disc's Worst Enemy
Rotation combined with forward flexion is the movement pattern most likely to herniate a disc.
Happens during everyday activities—lifting suitcase into car, twisting to reach something while bent, picking up toddler while turning.
Rule: pivot your feet, don't twist your spine.
If you need to turn while holding something, turn your whole body. Move your feet. Keep shoulders and hips aligned. Never rotate through lumbar spine while bent forward or holding weight.
That one rule prevents more disc injuries than any other single intervention.
When to Seek Professional Assessment After Recovery
Maintenance care's proactive, not reactive.
Waiting till pain returns means you've crossed from maintenance into treatment. Goal's catching dysfunction early.
Routine Maintenance Timeline
After completing recovery, baseline assessment 30-60 days later establishes your new functional standard.
Assessment measures:
- Range of motion symmetry
- Postural alignment
- Compensatory movement patterns
- Core activation quality
- Gait mechanics
From there, quarterly check-ups first year allow early detection of compensatory patterns. After one year stability, biannual assessments are sufficient after one year of stability.
The 15-minute disc restoration protocol at Touch of Wellness Chiropractic was built around this maintenance model—efficiency paired with clinical precision.
Red Flags That Require Immediate Assessment
Not all pain's a red flag, but certain symptoms indicate nerve involvement or structural compromise.
- Radiating leg pain following dermatomal pattern
- Numbness or tingling persisting beyond a few minutes
- Progressive weakness in specific muscle group
- Pain worsening with rest or lying down
- Loss of bowel or bladder control (emergency—seek care immediately)
These require professional evaluation within 48 hours. They indicate potential nerve compression or structural instability that won't resolve with rest or exercise.
If you're experiencing nerve-related symptoms that don't match typical muscle soreness pattern, that's a diagnostic signal—not something to wait out.
The Difference Between Soreness and Re-Injury
Muscle soreness is dull, improves with movement, resolves in 24-48 hours.
Disc or nerve pain is sharp, worsens with specific movements like bending or sitting, often radiates down leg.
If you can't clearly distinguish between them, err on assessment side.
| Symptom Characteristic | Normal Muscle Soreness | Disc/Nerve Problem |
|---|---|---|
| Pain quality | Dull, achy, diffuse | Sharp, stabbing, or burning with clear location |
| Location | Bilateral, muscle belly | Unilateral, radiating down leg in dermatomal pattern |
| Movement response | Improves with gentle movement | Worsens with flexion, sitting, or specific positions |
| Duration | Resolves in 24-48 hours | Persists beyond 48 hours or progressively worsens |
| Morning vs. evening | Worse in morning, improves through day | Worse after prolonged sitting or at end of day |
| Response to rest | Improves with rest | May worsen with rest or lying flat |
What a Maintenance Visit Actually Looks Like
Maintenance visit's not a treatment session.
It's functional movement assessment, posture evaluation, identification of compensatory patterns. If dysfunction's found, it's corrected. If everything's functioning well, you leave with confirmation your maintenance plan's working.
Visit includes:
- Movement screening to identify asymmetries
- Posture analysis for compensatory shifts
- Manual assessment of spinal segments for restricted motion
- Core activation testing
- Gait evaluation
If a problem's identified, it's addressed on the spot—usually single adjustment, mobility drill, or corrective exercise cue. If nothing's found, you walk out knowing your maintenance plan's sufficient.
That's the difference between maintenance and treatment. Treatment fixes a problem. Maintenance confirms there isn't one.
FAQ
How often should I get a chiropractic check-up after my disc has healed?
The goal of maintenance is independence, not dependence.
After completing recovery, periodic check-ups serve a diagnostic function—identifying early biomechanical issues before they produce symptoms. Proactive assessment, not ongoing treatment.
Most patients benefit from baseline assessment 30-60 days after completing recovery, then quarterly check-ups first year. After one year stability, biannual assessments are sufficient.
If you're managing your maintenance plan correctly, check-ups confirm that. If something's drifting, they catch it early. Either way, you're not there because you need treatment. You're there preventing the need for treatment.
What are the three most important exercises for preventing disc re-injury?
Transverse abdominis activation (bracing), glute bridges for posterior chain strength, and bird-dog for core stability without spinal flexion.
These three address primary mechanisms of disc protection: intra-abdominal pressure, posterior chain support, and reflexive stabilization.
Bracing creates rigid cylinder around spine preventing shear and compression from reaching discs. Glute bridges rebuild posterior chain counterbalancing forward spinal load. Bird-dog trains nervous system to maintain neutral spine during asymmetrical movement.
Everything else is supplemental. These three are foundational.
Can I return to high-impact activities like running after a disc injury?
Returning to high-impact activities requires sufficient core stability and proper biomechanics to absorb shock effectively.
This isn't yes-or-no—it's assessment-based decision depending on your specific injury, recovery timeline, and current functional capacity.
Running places repetitive compressive forces on spine. If core can't stabilize reflexively and glutes aren't strong enough to absorb impact, those forces transfer directly to discs. That's re-injury waiting to happen.
But if you've rebuilt necessary stability and strength, and you can demonstrate proper gait mechanics without compensation, running's manageable. Key's rebuilding foundation before reloading structure.
Shockwave Therapy can sometimes accelerate tissue remodeling for patients working toward high-impact activity clearance, but it's not a substitute for proper motor patterning.
What's the difference between normal muscle soreness and a disc pain flare-up?
Muscle soreness is dull, improves with movement, resolves within a day or two.
Disc or nerve pain is sharp, radiating, worsens with specific movements like bending or prolonged sitting.
If pain doesn't follow muscle soreness pattern, it requires professional evaluation. Disc pain often has mechanical trigger—specific movement or position reproducing it. Muscle soreness doesn't. It's generalized and diffuse.
If you bend forward and feel sharp, localized pain radiating into leg, that's not soreness. That's biomechanical issue. Stop the activity and get it assessed.
What is the single worst habit for disc health?
Prolonged static sitting with poor posture.
This position flexes lumbar spine and places consistent pressure on posterior discs, where they're most vulnerable to herniation.
Movement breaks and lumbar support are non-negotiable if work requires extended sitting. Set a timer. Stand every 20-30 minutes. Reset posture. Use lumbar roll. These aren't optional if you want to maintain disc health long-term.
The concept of Back School—educational programs teaching patients spinal mechanics and ergonomics for self-care—exists because this pattern's so pervasive and damaging.
Does maintenance mean I'll be doing these exercises forever?
Core stabilization exercises become part of your baseline fitness routine—not temporary fix.
Once motor patterns are established and strength's built, maintaining them requires significantly less time than building them initially. Most patients spend 10-15 minutes daily on targeted exercises after first 3-6 months.
That's not "forever" in burdensome sense. That's what it takes to keep your spine functioning how it's supposed to. Same as brushing teeth—maintenance preventing much bigger problem.
What if a maintenance exercise consistently causes pain?
If an exercise isn't working, answer isn't pushing through it.
Stop. Reassess the form or the exercise itself.
Pain during maintenance exercise means something's wrong—either movement pattern's incorrect, or that specific exercise isn't appropriate for your biomechanics. Both are fixable, but not by ignoring the signal.
This is where willingness to stop and reassess becomes clinical standard. If something isn't producing intended result, repeating it doesn't make it effective. It makes it destructive.
How do I know if my core is actually activating during exercise?
Proper transverse abdominis activation creates intra-abdominal pressure—you should feel midsection tighten and expand slightly, not suck in.
If you can't consciously create this bracing sensation, core isn't activating effectively, which means exercise isn't protecting spine how it should.
Test it: Place hands on lower abdomen. Take breath in. Now brace like you're about to take punch. You should feel abdomen push out against hands—not pull in. That outward pressure's the signal transverse abdominis is firing correctly.
If you feel abs hollow or pull inward, you're recruiting wrong muscles. That's rectus abdominis contraction, which doesn't stabilize spine.
Same principle applies to stress on your cervical spine—proper muscle activation protects structure, improper activation accelerates breakdown.
Conclusion
Most disc injuries return not because the recovery plan failed.
They return because the patient stopped doing what made recovery possible.
Maintenance isn't optional. It's the difference between recovering once and staying recovered.
You invested time, effort, money into restoring disc function. That investment only pays long-term dividends if you protect it. The exercises, the spinal hygiene, the periodic assessments—these aren't extras. They're the maintenance contract on the progress you made.
Your spine doesn't care about intentions. It responds to mechanical load you place on it every single day. If that load's controlled, progressive, biomechanically sound, discs stay healthy. If it's not, they break down—whether you feel it or not.
You've got the tools. You know the patterns.
Question isn't whether maintenance works. Question's whether you'll commit to doing it.
If your disc's healed but you're unsure whether your maintenance plan's actually protecting you—that's worth a real conversation.
An assessment at Touch of Wellness Chiropractic identifies compensatory patterns and early biomechanical stress before they produce symptoms. Not ongoing treatment. Diagnostic verification that what you're doing is working.
If you're in Morton, Peoria, or the surrounding area and want to confirm your maintenance plan's sufficient, find out what your assessment includes.
Recovery got you to the finish line. Maintenance is what keeps you there.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet