
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
Disc Recovery vs. Spinal Fusion: What Morton, IL Patients Need to Know
Non-invasive disc recovery aims to restore function by addressing the root cause of disc issues—nervous system dysfunction and compromised spinal mechanics—using chiropractic adjustments and advanced therapies like decompression, shockwave therapy, and targeted strengthening. Spinal fusion surgery is an invasive procedure that permanently joins two or more vertebrae to eliminate motion at a problem segment, typically recommended when a physician believes conservative measures have failed or for severe spinal instability. The fundamental difference isn't just surgical versus non-surgical. It's whether you're trying to restore the system that failed or surgically remove the symptom that system produced.
Spinal fusion treats the disc as the problem. Non-invasive disc recovery treats the disc as a symptom of the system that failed. One approach locks the breakdown in place. The other asks why it broke down. Your disc didn't just decide to herniate one day. Something broke down in the way your spine moves, loads weight, and communicates with your nervous system. The goal with non-invasive care is to decompress the affected segment, restore proper motion to the surrounding vertebrae, and retrain the nervous system to stabilize the area correctly. One approach asks why the system failed. The other decides the system can't be trusted and shuts it down.
This article walks through what each approach actually does, what recovery looks like, what the long-term risks are, and how to know which path makes sense for your specific situation. If you're sitting in Morton, Peoria, or anywhere in central Illinois with a surgical recommendation in hand and no clear understanding of what your other options are, this is the conversation you need to have before you make that decision.
Last Updated: April 30, 2026
- What Non-Invasive Disc Recovery Actually Does
- What Spinal Fusion Surgery Actually Does
- Recovery Time: Surgery vs. Non-Invasive Care
- Long-Term Risks You Need to Understand
- When Your Doctor Says Surgery Is the Only Option
- Who Shouldn't Choose the Non-Invasive Path
- How to Know If You're a Candidate
- Frequently Asked Questions
- The Real Question Isn't Which One Works—It's Which One Fits Your Case
What Non-Invasive Disc Recovery Actually Does
Most people think a herniated disc is the problem. It's not.
It's what happens when the system that's supposed to protect the disc stops working. Your disc doesn't have its own blood supply once you're past childhood. It gets nutrients through diffusion from the surrounding tissue when the spine moves correctly. When the vertebrae above and below that disc stop moving the way they should—because of injury, postural breakdown, or chronic misalignment—the disc stops getting what it needs.
It dries out. It weakens. And eventually it bulges or herniates under normal load.
The Nervous System Connection
Your spine isn't just holding you upright. It's running the whole system.
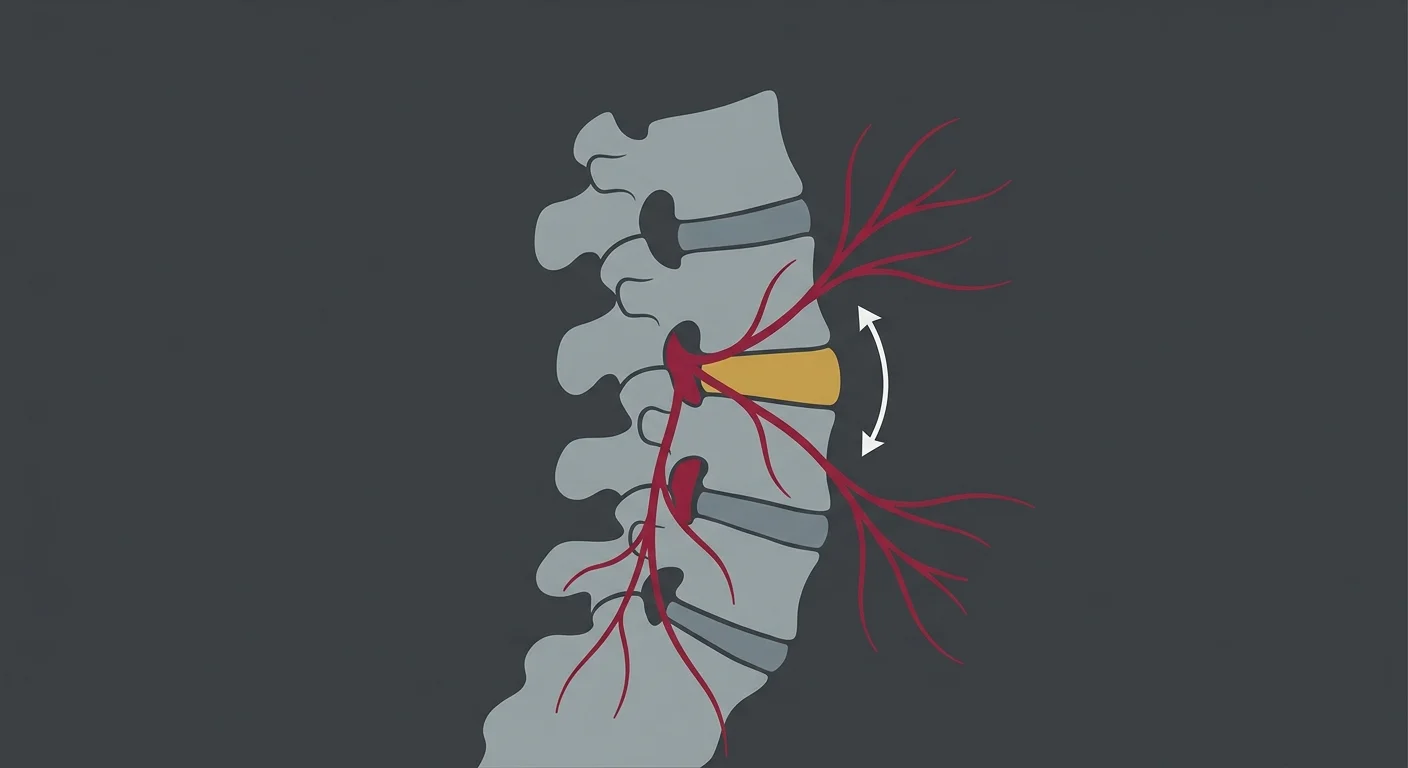
It houses your spinal cord and the nerve roots that branch out to every part of your body. When a disc herniates, it's usually pressing on one of those nerve roots. That's what produces the radiating pain, the numbness, the tingling down your leg.
But here's what most people don't understand: the disc pressed on the nerve because the vertebrae shifted out of their normal position. And the vertebrae shifted because the muscles, ligaments, and nervous system that control spinal stability stopped doing their job correctly.
A chiropractic adjustment doesn't push the disc back in. It restores normal motion to the vertebrae that aren't moving, which reduces the mechanical pressure on the disc and nerve. When the pressure drops, inflammation drops. When inflammation drops, pain drops. And when the nervous system isn't getting constant pain signals, it stops bracing the entire area—which lets the muscles relax and the healing process actually start.
That's not theoretical. That's documented in clinical studies on patients with lumbar radiculopathy—nerve pain caused by disc issues—who improved through chiropractic management without surgery.
How Chiropractic Adjustments Decompress the Disc
The adjustment itself is specific. It's not a generalized "crack your back and hope for the best" move.
I use manual adjustments and techniques like flexion-distraction—a gentle, rhythmic motion applied to the lower back that creates a pumping action in the disc. That pumping action does two things: it pulls the bulging portion of the disc away from the nerve, and it helps nutrients flow back into the disc tissue.
Flexion-distraction doesn't feel like what most people imagine when they think of chiropractic. There's no twisting, no popping. It's a slow, controlled stretch applied over several minutes while you're lying face-down on a specialized table. The table itself moves in sync with the adjustment to create the decompression effect.
If you want to understand the full mechanical process behind how non-invasive disc recovery works at the spinal and nervous system level, that article walks through each step in detail.
Not every disc case needs flexion-distraction. Some respond better to side-posture adjustments or instrument-assisted techniques. The method gets picked based on what your body's telling me during the exam—not based on what I did for the last patient who walked in.
Advanced Modalities That Support Disc Healing
The adjustment handles the mechanical side. But if the tissue around the disc is inflamed, scarred, or weakened, you need more than just restored motion.
That's where advanced therapies come in.
Shockwave Therapy delivers high-energy acoustic waves directly into damaged tissue. It breaks up scar tissue, stimulates blood flow, and triggers the body's natural repair response. For disc cases, it's used on the muscles and ligaments surrounding the affected segment—the ones that've been compensating for months or years while the disc was breaking down.
Cold Laser Therapy reduces inflammation at the cellular level. It's not heat. It's focused light energy that penetrates deep into the tissue and speeds up the healing process without any sensation during treatment.
Then there's the exercise component. A disc that's been unstable for months doesn't just magically restabilize because you adjusted it twice. You've got to retrain the muscles that're supposed to hold it in place. That means targeted core strengthening, hip mobility work, and postural retraining.
Not generic stretches you found on YouTube. Specific exercises based on where your movement patterns broke down.
What "Restoring Function" Actually Means
Here's what non-invasive disc recovery doesn't do: it doesn't make the herniation disappear on an MRI.
Some herniations do shrink over time. Some don't.
What matters is whether you can move without pain, sleep through the night, and get back to the activities that define your life. If that's happening, the MRI is irrelevant.
The goal is decompression, stability, and nervous system reset. If the nerve isn't being compressed, if the segment is moving correctly, and if your nervous system isn't stuck in a chronic pain loop, you've recovered. The herniation might still show up on imaging.
That doesn't mean the treatment failed. It means your body adapted.
| Dysfunction Addressed | How It's Treated | Expected Outcome |
|---|---|---|
| Restricted spinal motion | Manual chiropractic adjustment, flexion-distraction | Improved segmental mobility, reduced disc pressure |
| Nerve compression and inflammation | Spinal decompression, Cold Laser Therapy | Decreased radiating pain, restored nerve function |
| Weakened stabilizing muscles | Targeted exercises, postural retraining | Long-term stability, reduced re-injury risk |
| Scar tissue and adhesions | Shockwave Therapy, soft tissue work | Improved tissue flexibility, better healing response |
What Spinal Fusion Surgery Actually Does
Spinal fusion is exactly what it sounds like.
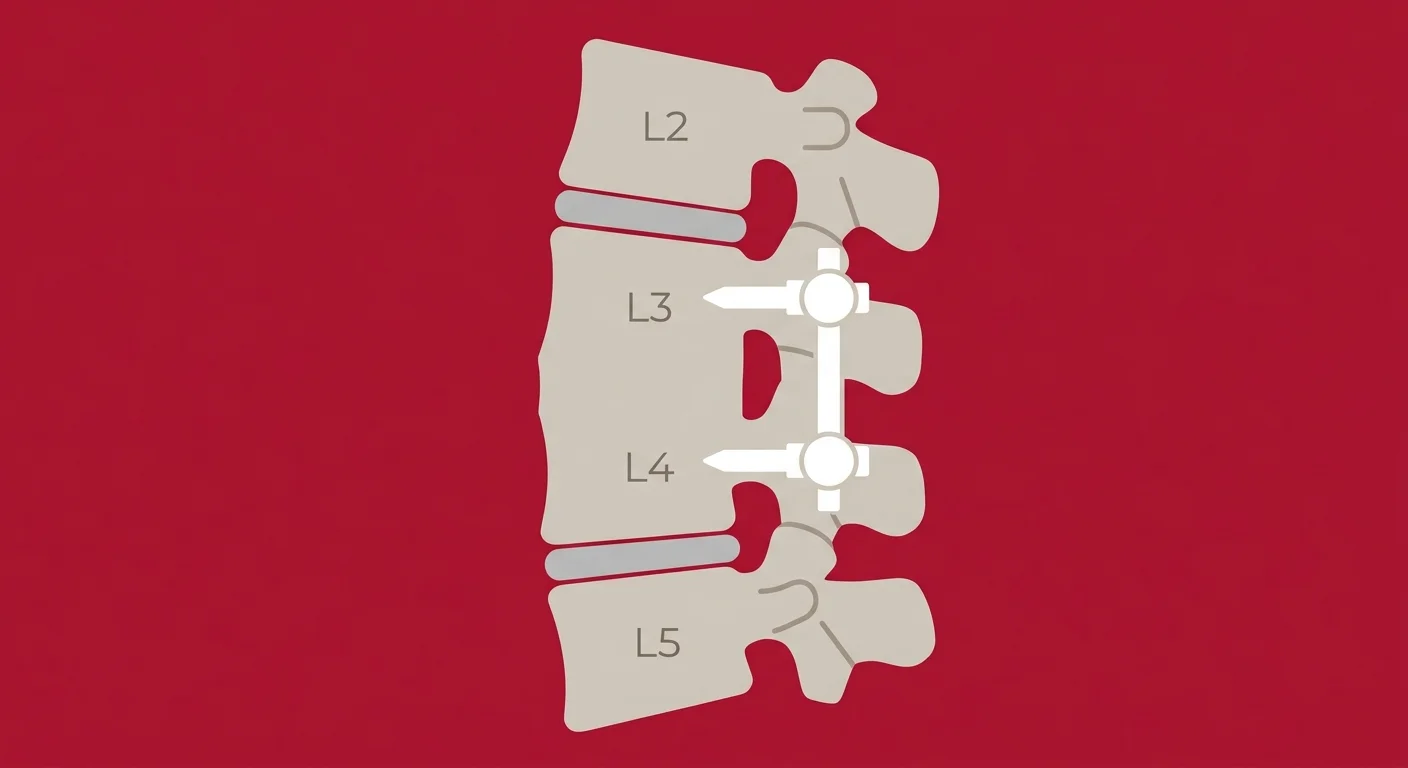
Two or more vertebrae are permanently joined together so they can no longer move independently. The surgeon removes the damaged disc, places a bone graft between the vertebrae, and inserts metal hardware—rods, screws, plates—to hold everything in place while the bone grows together.
Once the fusion is complete, that section of your spine is locked. It doesn't flex. It doesn't rotate. It's structurally stable, but it's also structurally rigid.
The motion that segment used to handle gets transferred to the vertebrae above and below the fusion.
According to the Mayo Clinic's overview of spinal fusion, the procedure is typically recommended for conditions like severe spinal instability, spondylolisthesis (where one vertebra slips forward over another), or degenerative disc disease that hasn't responded to conservative treatment.
Why Surgeons Recommend Fusion
Surgeons aren't wrong to recommend fusion in certain cases.
If your spine is structurally unstable—meaning the vertebrae are shifting in ways that could damage the spinal cord or nerves permanently—fusion is the appropriate intervention. If you have a deformity like scoliosis that's progressing and affecting your ability to breathe or move, fusion is the standard surgical intervention.
The problem is that "hasn't responded to conservative treatment" is a subjective standard.
What counts as conservative treatment? Six weeks of physical therapy? Three months of over-the-counter pain meds and rest? A few visits to a chiropractor who ran the same adjustment protocol on every patient regardless of presentation?
If the conservative treatment didn't address the root cause—the mechanical dysfunction and nervous system breakdown that caused the disc to fail—then of course it didn't work. That doesn't mean surgery is the only option left.
It means the right conservative treatment hasn't been tried yet.
What Happens During the Surgery
The surgery itself is significant.
You're under general anesthesia for several hours. The surgeon makes an incision—either through your back or, in some cases, through your abdomen to access the spine from the front. The damaged disc is removed entirely. A bone graft is placed in the empty space. That graft can come from your own pelvis, from a donor, or from synthetic material.
Then the hardware goes in. Screws are drilled into the vertebrae above and below the disc. Rods connect the screws to hold everything rigid while the bone graft fuses to the vertebrae over the next several months.
Recovery from the surgery itself is just the beginning. You're looking at a hospital stay of a few days, then weeks of restricted movement. No bending. No twisting. No lifting anything heavier than a gallon of milk.
Physical therapy starts after the initial healing phase, but the goal isn't to restore motion to that segment—it's to teach you how to move with a fused spine.
The Problem Fusion Doesn't Solve
Spinal fusion removes motion from a segment that's causing pain.
What it doesn't do is address why that segment failed in the first place.
The mechanical dysfunction and nervous system breakdown that caused the disc to herniate are still there. You've just locked the symptom in place. The vertebrae above and below the fusion now have to absorb all the motion that the fused segment used to handle.
And over time, those segments start to break down faster than they would've otherwise.
That's called adjacent segment disease. It's not a rare complication. It's a documented, predictable outcome in a significant percentage of fusion patients. A peer-reviewed study in The Bone & Joint Journal tracking long-term outcomes after lumbar fusion found that many patients experienced new disc problems in the segments neighboring the fusion within 10 years.
When that happens, the options are limited. You can't go back and unfuse the spine.
The next step is usually another fusion. And then the cycle continues.
Recovery Time: Surgery vs. Non-Invasive Care
The word "recovery" means something different depending on which path you take.
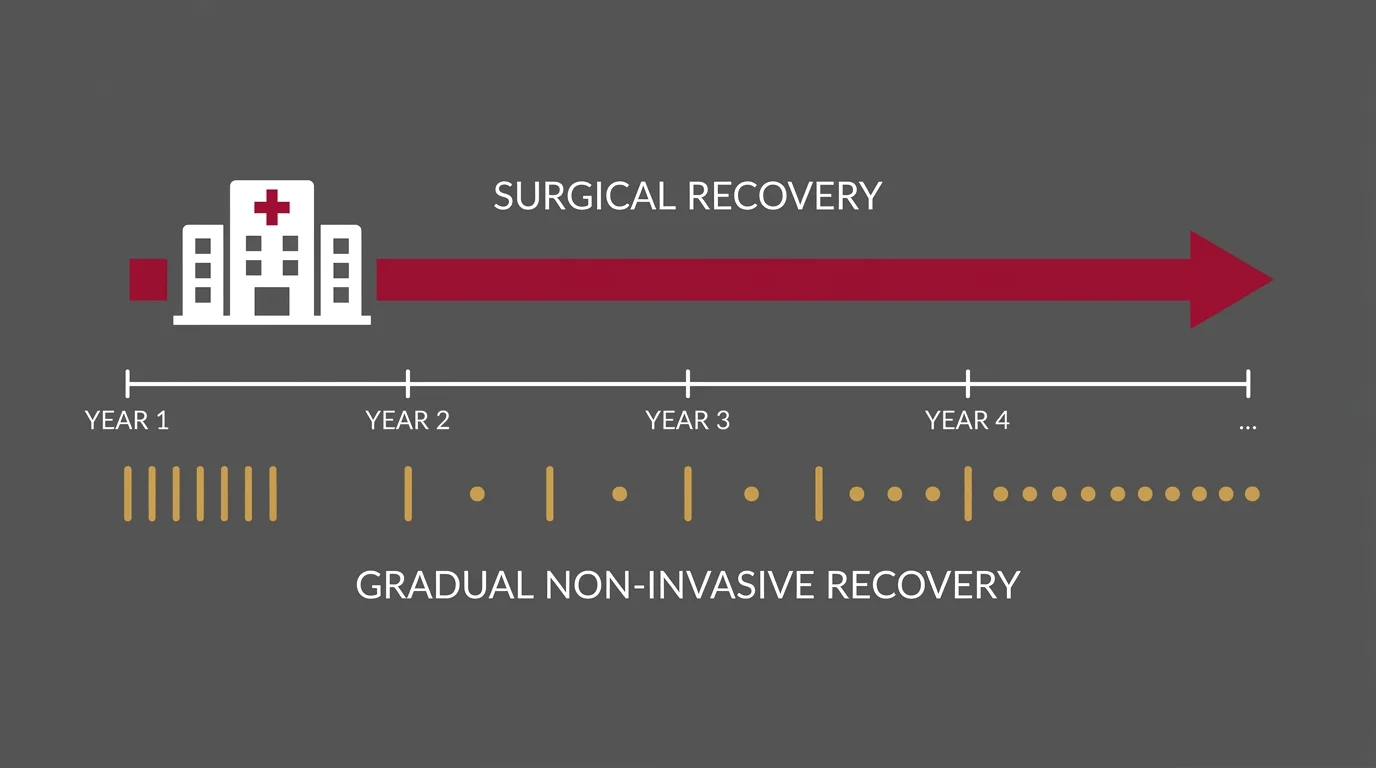
With surgery, recovery is structural. With non-invasive care, recovery is functional. Those aren't the same thing.
When a surgeon says you've recovered from spinal fusion, they mean the bone has fused, the hardware is stable, and the surgical site has healed. That takes six months to a year.
When I say you've recovered from a disc injury, I mean you can move without pain, you've returned to normal activity, and the segment is stable enough that your body can manage it on its own. That timeline varies—but functional recovery often happens faster than surgical recovery, and it doesn't require removing you from your life for months at a time.
| Milestone | Spinal Fusion | Non-Invasive Disc Recovery | Notes |
|---|---|---|---|
| Hospital stay | 2–5 days post-surgery | None — outpatient care only | Fusion requires immediate post-op monitoring; non-invasive patients go home after each visit. |
| Return to light activity | 6–12 weeks (with restrictions) | 2–6 weeks (often sooner with modifications) | Fusion patients can't bend, twist, or lift during early healing; non-invasive patients maintain modified activity throughout. |
| Return to work (desk job) | 4–8 weeks minimum | 1–2 weeks (often maintained throughout care) | Depends on pain tolerance and physical demands. Fusion requires extended leave; non-invasive patients often continue working. |
| Return to physical work | 3–6 months (if cleared) | 6–12 weeks (progressive return) | Heavy lifting and repetitive bending are restricted longer after fusion. Non-invasive recovery focuses on gradual load tolerance. |
| Full structural healing | 6–12 months (bone fusion complete) | N/A — goal is functional stability, not structural change | Fusion success is measured by bone growth. Non-invasive success is measured by pain reduction and restored movement. |
| Long-term physical therapy | Ongoing to compensate for lost motion | Maintenance exercises after active care ends | Fusion patients need lifelong movement strategies. Non-invasive patients transition to self-managed stability work. |
What "Recovery" Actually Means in Each Case
For spinal fusion, recovery is about bone healing and hardware stabilization. It's structural.
The goal is for the bone graft to fuse to the vertebrae and for the hardware to stay in place without complications. That process takes months, and during that time, you're restricted from most normal activities. You're not recovering your ability to move—you're recovering from the surgery itself.
For non-invasive disc recovery, the goal is progressive restoration of function. You're not waiting for bone to fuse. You're working to decompress the nerve, restore motion to the fixated segments, and retrain the nervous system to stabilize the area.
Progress is measured by how you feel, how you move, and whether you can return to the activities that matter to you. Some patients see significant improvement within a few weeks. Others need several months.
But the timeline isn't determined by a surgical healing schedule—it's determined by your body's response to care.
The Return-to-Work Reality
If you've got a desk job, you might be cleared to return to work 4–8 weeks after spinal fusion—assuming there are no complications.
But you're returning with restrictions. No prolonged sitting without breaks. No bending forward at the waist. No lifting anything over 5–10 pounds.
If you've got a physical job—construction, nursing, warehouse work—you're looking at 3–6 months minimum before you're cleared to return to full duty. And even then, you're returning with a spine that no longer moves the way it used to.
The long-term accommodations are permanent.
With non-invasive disc recovery, most patients with desk jobs continue working throughout care—sometimes with ergonomic adjustments or modified schedules, but they're not out of work for months. Physical workers often return within 6–12 weeks, with a gradual increase in load tolerance as the segment stabilizes.
The difference isn't just time off. It's whether you're recovering your ability to do your job the way you used to, or whether you're learning to work around a permanent structural change.
Long-Term Risks You Need to Understand

Every medical decision carries risk.
The question is what kind of risk you're willing to accept—and what you get in return for taking it.
With surgery, the risks are immediate and long-term. Immediate risks include infection, nerve damage, blood clots, and anesthesia complications. Long-term risks include hardware failure, chronic pain at the surgical site, and adjacent segment disease.
Those aren't rare outliers. They're documented outcomes that happen to a significant percentage of fusion patients.
With non-invasive care, the primary risk isn't harm. It's time. If your case genuinely requires surgery and you delay too long trying conservative care, you could miss the window where surgery is still an option.
But that risk is manageable if you're working with a provider who knows when to refer out—and who isn't running the same protocol for months hoping it eventually works.
Surgical Risks: Immediate and Long-Term
The immediate surgical risks are the ones most people think about: infection at the surgical site, nerve damage during the procedure, blood clots forming in the legs and traveling to the lungs, adverse reactions to anesthesia.
Those are real, and they happen in a small but measurable percentage of cases.
Then there's hardware failure. The screws can loosen. The rods can shift. The bone graft can fail to fuse, leaving you with a "pseudarthrosis"—a false joint where the fusion was supposed to happen.
When hardware fails, the solution is usually another surgery.
But the bigger risk—the one that doesn't get enough attention during the initial surgical consultation—is adjacent segment disease. When you fuse two vertebrae, the segments above and below that fusion have to absorb all the motion the fused area used to handle.
Over time, those segments wear out faster. Discs degenerate. Arthritis accelerates.
And within 10 years, many fusion patients are dealing with new disc problems in the segments next to the original fusion.
The NIH defines Failed Back Surgery Syndrome as persistent or recurring pain after spinal surgery—and it's more common than most patients realize before they sign the consent form.
Non-Invasive Risks: What Can Go Wrong
The most common fear people have about chiropractic care for disc issues is: "What if you make it worse?"
When chiropractic care is performed by a qualified Doctor of Chiropractic after a thorough assessment, the risk of making a disc herniation worse is extremely low. I don't use aggressive force. I don't twist you into positions your spine can't tolerate.
The techniques used for disc cases—flexion-distraction, instrument-assisted adjustments, gentle manual mobilization—are specifically designed to decompress, not compress.
The real risk with non-invasive care is wasted time. If your case genuinely requires surgery—because you've got progressive neurological deficits, severe instability, or a condition like cauda equina syndrome—and you spend months trying conservative care that isn't appropriate for your situation, you could end up in a worse position than if you'd gone straight to surgery.
That's why the assessment matters. A competent chiropractor doesn't promise to restore everything. They assess your case, tell you honestly whether it's something they can help with, and refer out if it's not.
If you're working with someone who guarantees results before they've even examined you, that's a red flag.
| Risk Category | Spinal Fusion | Non-Invasive Disc Recovery |
|---|---|---|
| Immediate complications | Infection, nerve damage, blood clots, anesthesia reactions | Temporary soreness, minor symptom flare-up during initial care (rare) |
| Hardware-related issues | Screw loosening, rod migration, pseudarthrosis (failed fusion) | Not applicable |
| Long-term structural changes | Adjacent segment disease, accelerated degeneration in neighboring discs | None — natural spinal motion preserved |
| Chronic pain outcomes | Failed Back Surgery Syndrome, persistent surgical site pain | Incomplete recovery if root cause not fully addressed |
| Time-related risk | Extended recovery period, prolonged activity restrictions | Delayed surgical intervention if case requires it and conservative care is prolonged |
When Your Doctor Says Surgery Is the Only Option

Your doctor isn't wrong to recommend surgery.
They're working from the model they were trained in. But "surgery is the only option" and "surgery is the standard first-line treatment" are two very different statements.
Most primary care physicians don't have training in functional chiropractic care. Medical school curriculum doesn't include coursework on spinal manipulation, nervous system-based disc recovery, or the evidence base for conservative management of herniated discs.
That's not a criticism—it's just a fact.
When your GP says there's nothing else to try, they're usually saying there's nothing else they know how to do.
Why GPs Often Skip the Chiropractic Conversation
The medical education system doesn't train doctors to think in terms of mechanical dysfunction.
It trains them to diagnose pathology and match it to a treatment protocol. If the diagnosis is "herniated disc" and the protocol options are "medication, physical therapy, or surgery," and the first two didn't work, the third one is what's left.
Functional chiropractic care doesn't fit cleanly into that model because it's not treating a pathology. It's correcting a mechanical breakdown. That requires a different diagnostic lens—one most GPs don't have because they were never trained in it.
According to the American Academy of Family Physicians' guidelines on lumbar disc herniation management, conservative care—including spinal manipulation—is the recommended first-line approach for most disc cases.
But "recommended" and "commonly implemented" aren't the same thing. Many GPs skip straight to imaging, pain meds, and surgical referrals because that's the pathway they're comfortable with.
What a Second Opinion Actually Looks Like
A chiropractic assessment for a disc case isn't a five-minute consultation where someone tells you they can restore you without even examining you.
It's a comprehensive evaluation.
I start with your history. How long has this been going on? What makes it better or worse? Have you had imaging? What treatments have you tried, and what happened?
Then I run orthopedic and neurological tests—checking reflexes, muscle strength, sensation, range of motion. If you've got an MRI or X-ray, I review it. If you don't, I determine whether imaging is necessary before moving forward.
The goal of that assessment isn't to sell you a 12-month care plan. It's to determine whether your disc problem is something that can be managed conservatively or whether you need a surgical consult.
If the assessment reveals progressive neurological deficits, severe instability, or a condition that's beyond the scope of chiropractic care, you'll be referred out. If it reveals mechanical dysfunction that's producing nerve compression and pain, you'll get a realistic care plan with measurable benchmarks and a clear timeline.
If you're sitting with a surgical recommendation and you're not sure whether you've actually exhausted your conservative options, that assessment is the conversation you need to have. Not because chiropractic is always the answer—but because when a primary care physician recommends surgery, you deserve to know what else exists before you make a permanent structural change to your spine.
Unexplained Doesn't Mean Untreatable
One of the most frustrating things patients hear from their doctors is some version of: "We've tried everything. There's nothing else we can do except surgery."
Here's the thing: "everything" usually means medication, rest, and maybe a few weeks of generic physical therapy.
That's not everything. That's the standard medical playbook for disc issues. If that playbook didn't work, it doesn't mean nothing will work. It means the approach that was tried didn't address the root cause.
Unexplained doesn't mean untreatable. It means no one's looked at the right thing yet.
If your disc herniated because the vertebrae above and below it stopped moving correctly, and no one ever addressed that mechanical restriction, then of course the disc didn't heal. You can't restore a movement problem with rest and pain meds.
A nervous system-based approach looks at why the disc failed—not just at the disc itself. And when you address the why, the body often has a remarkable ability to adapt and recover.
Not always. Not in every case. But often enough that writing off conservative care as "already tried" based on a few weeks of ineffective treatment is premature.
Who Shouldn't Choose the Non-Invasive Path

Non-invasive disc recovery requires full clinical and financial commitment.
Partial commitment produces partial results—and when the results are partial, that validates the belief that surgery was the only real option all along.
If you're not willing to follow the full care plan, this isn't for you.
That's not a sales pitch. That's a clinical reality. Disc recovery is a process. It requires consistent appointments, targeted exercises between visits, and sometimes modifications to how you move and work during the recovery phase.
If you're going to pick and choose which parts of the plan to follow—cancel appointments when you feel better for a week, skip the exercises, ignore the postural corrections—you're setting yourself up for incomplete recovery. And that's not fair to either of us.
If You're Not Willing to Follow the Full Care Plan
Disc recovery doesn't work like a prescription. You can't take half the dose and expect full results.
If you're coming in for adjustments but skipping the exercises, you're addressing half the problem. The adjustment restores motion and decompresses the nerve, but if the muscles that're supposed to stabilize the segment don't get retrained, the instability comes back.
If you're doing the exercises but canceling appointments when your pain drops for a few days, you're not giving the nervous system enough input to reset. The pain reduction is temporary because the root cause hasn't been fully corrected yet.
This isn't about compliance for compliance's sake. It's about the fact that disc recovery is a multi-step process, and if you skip steps, the process doesn't complete. If something isn't working after a few visits, we change it.
But if you're not following the plan long enough to know whether it's working, there's nothing to change. You're just guessing.
If You Need Immediate Structural Stabilization
Some cases require surgery.
Not because conservative care is inferior, but because the condition has progressed past the point where a non-invasive approach is safe or appropriate.
If you've got severe spinal instability—meaning your vertebrae are shifting in ways that could damage the spinal cord—that's a surgical case. If you've got progressive neurological deficits like foot drop, where you're losing motor function because the nerve is being compressed too severely for too long, that's a surgical emergency.
If you've got cauda equina syndrome—a rare but serious condition where the nerves at the base of the spinal cord are compressed, causing loss of bowel or bladder control—you need surgery immediately.
Any competent chiropractor will tell you that on day one. My job isn't to avoid surgery at all costs. It's to determine whether your case can be managed conservatively or whether a surgical consult is warranted.
If you need surgery, you'll be referred out. If you don't, you'll get a care plan that addresses the root cause.
If You're Looking for a One-Visit Solution
Disc recovery takes weeks to months.
If you're expecting one adjustment to resolve a problem that developed over years, you're setting yourself up for disappointment and wasted money.
The first visit does something. Most patients leave with reduced pain or improved range of motion. But that's not recovery—that's decompression. Recovery is when the segment stabilizes enough that your body can manage it on its own.
That requires multiple visits, consistent input to the nervous system, and time for the tissue to adapt.
If you're not willing to commit to that timeline, you're not a good fit for this approach. And that's fine. But don't start the process, bail after two visits because you're not 100% better, and then conclude that chiropractic doesn't work.
It works when it's applied correctly, consistently, and long enough for the body to respond.
How to Know If You're a Candidate

Candidacy isn't determined by a phone call or a quick online form.
It's determined through a comprehensive assessment—history, exam, review of imaging if available, and a frank conversation about whether your case is something that can be managed conservatively or whether it's crossed into surgical territory.
Not every disc case is a chiropractic case. Some are surgical cases from the start. Some start as conservative care candidates but don't respond and need to be referred out.
The assessment is where that gets sorted out—and it happens before any care plan is presented, before any financial commitment is made.
What the Initial Assessment Covers
The assessment starts with your history.
How long has the pain been going on? Where exactly does it radiate? Is there numbness or tingling? Weakness in the leg? Does it get worse with certain movements—bending forward, sitting, standing up from a chair? Have you had imaging done, and if so, what did it show?
Then I run orthopedic and neurological tests. I check your reflexes, muscle strength, and sensation. I test range of motion in your spine and hips. I run specific tests—straight leg raise, slump test, Kemp's test—designed to identify whether the pain is coming from the disc, the nerve, or the surrounding joints and muscles.
If you've got an MRI or X-ray, I review it. If you don't have imaging and the exam findings suggest it's necessary, I'll refer you for it before moving forward.
The goal isn't to skip imaging—it's to use it appropriately. Some cases need it. Some don't. The exam determines which category you're in.
Realistic Expectations: What Non-Invasive Care Can and Can't Do
Non-invasive disc recovery isn't about making the herniation disappear on an MRI.
It's about decompressing the nerve, restoring enough function that the body can adapt, and getting you back to the activities that define your life.
Some herniations do shrink over time. Some don't. What matters is whether you can move without pain, sleep through the night, and do your job without constant discomfort.
If that's happening, the MRI doesn't matter. The herniation might still be there. But if the nerve isn't being compressed, if the segment is moving correctly, and if your nervous system has stopped sending constant pain signals, you've recovered functionally—even if the imaging doesn't look perfect.
The care plan is built from what you report during treatment, not from what the MRI shows. If you're improving—less pain, better movement, returning to normal activities—the plan continues. If you're not improving after a reasonable trial, the plan changes.
And if it becomes clear that your case requires a surgical consult, you'll get an honest care assessment that tells you that—not six months of repeated adjustments hoping something eventually clicks.
If It Isn't Working, We Change It
A core principle at Touch of Wellness Chiropractic is reassessment.
If a treatment isn't working after a few visits, we change it. We don't repeat the same protocol for months and hope for a different result.
That might mean switching from flexion-distraction to manual adjustments. It might mean adding Shockwave Therapy to break up scar tissue that's limiting motion. It might mean referring you to a different specialist if what you're dealing with is outside the scope of chiropractic care.
The willingness to pivot isn't a weakness—it's the whole point.
If your case genuinely requires a surgical consult, I'll be the first to tell you. Not because I'm giving up, but because some cases need surgery and pretending they don't doesn't serve anyone.
The goal is to get you better—not to avoid surgery at all costs. If surgery is the right call, you'll get an appropriate referral. If it's not, you'll get a care plan that addresses the root cause and gives your body a real chance to recover.
If you've been dealing with chronic or recurring pain that your doctor has dismissed or written off as something you'll just have to live with, that's worth investigating. Not every case is fixable.
But a lot of them are—if someone's willing to look at the system instead of just the symptom.
Frequently Asked Questions
What is the typical recovery time for spinal fusion vs. non-invasive disc recovery?
Spinal fusion recovery is measured in months.
The bone graft needs 6–12 months to fully fuse to the vertebrae. During that time, you're restricted from most normal activities—no bending, no twisting, no lifting. You might be cleared to return to light activity at 6–12 weeks, but full structural healing takes closer to a year.
Even after the fusion is complete, you're living with a spine that no longer moves the way it used to.
Non-invasive disc recovery is gradual, but functional improvement often happens much sooner. Some patients notice reduced pain and better movement within a few weeks. Full recovery—meaning you're back to normal activity without constant discomfort—can take 8–16 weeks depending on the severity of the disc issue and how your body responds to care.
The timeline isn't determined by a surgical healing schedule. It's determined by how quickly the nervous system resets and the segment stabilizes.
Can a chiropractor make a herniated disc worse?
When performed by a qualified Doctor of Chiropractic after a thorough assessment, the risk is extremely low.
I use specific, gentle techniques designed to decompress the spine and nerve—not aggressive force. Flexion-distraction, instrument-assisted adjustments, and manual mobilization are all designed to reduce pressure on the disc, not increase it.
The bigger risk isn't that chiropractic will make the disc worse. It's that a patient will go to someone who doesn't do a proper assessment, who runs the same protocol on every patient regardless of presentation, and who doesn't know when to stop and reassess if something isn't working.
That's not a chiropractic problem—that's a competence problem. And it exists in every field.
What are the main risks of spinal fusion surgery?
Immediate risks include infection, nerve damage, blood clots, and adverse reactions to anesthesia.
Those happen in a small percentage of cases, but they're real.
Long-term risks are more common. Hardware can fail—screws loosen, rods shift, bone grafts don't fuse correctly. When that happens, you need another surgery to address it. Then there's adjacent segment disease: the vertebrae above and below the fusion wear out faster because they're absorbing all the motion the fused segment used to handle.
Many fusion patients end up dealing with new disc problems in those neighboring segments within 10 years.
According to Spine-health's overview of sciatica surgery considerations, fusion is appropriate for certain conditions—but it's not a risk-free solution, and the long-term consequences need to be part of the decision-making process before you sign the consent form.
What happens if I try non-invasive care and it doesn't resolve my disc issue?
If non-invasive care isn't producing results after a reasonable trial—usually 4–8 weeks depending on the severity—the plan changes.
That might mean adjusting the technique, adding advanced therapies, or referring you to a different specialist.
If it becomes clear that your case requires surgery, I'll tell you that and make an appropriate referral. The goal isn't to avoid surgery at all costs. The goal is to determine whether your disc problem can be resolved conservatively or whether surgical intervention is necessary.
If it's necessary, you'll get that answer early—not after six months of ineffective care.
How do I know if I'm a good candidate for non-invasive disc recovery?
Candidacy depends on the type and severity of your disc issue, your symptoms, and your overall health.
That's determined through a comprehensive chiropractic assessment—not a quick online form.
The assessment includes a history, physical exam, orthopedic and neurological testing, and review of any imaging you've had done. I use that information to determine whether your case is something that can be managed conservatively or whether it's crossed into surgical territory.
If you're a candidate, you'll get a realistic care plan with measurable benchmarks. If you're not, you'll get an appropriate referral.
Won't I just end up needing surgery anyway?
Some cases do eventually require surgery.
But many don't—and the difference is whether the root cause gets addressed or whether you're just managing symptoms until they get bad enough to operate.
If the mechanical dysfunction and nervous system breakdown that caused the disc to fail aren't corrected, the disc won't stabilize. You can mask the pain with medication, avoid certain movements, and hope it gets better on its own, but the underlying problem is still there.
That's the scenario where people end up in surgery after years of "trying everything."
If the mechanical dysfunction is corrected—if the fixated segments start moving again, if the nerve gets decompressed, if the muscles and ligaments get retrained to stabilize the area—the disc has a real chance to adapt and heal.
Not every case responds. But enough of them do that dismissing conservative care as "just delaying the inevitable" before it's even been tried is premature.
Is non-invasive disc recovery covered by insurance?
Coverage depends on your specific plan.
Touch of Wellness Chiropractic verifies insurance benefits before care begins, but verification is not a guarantee of payment. Some plans cover chiropractic care for disc-related conditions with no issues. Others have restrictions, co-pays, or limited visit allowances.
I also co-own Bushido Billing, which gives me direct billing literacy most providers don't have. That doesn't mean insurance will always pay—but it does mean you'll get an honest conversation about what your plan covers and what your out-of-pocket responsibility will be before you commit to care.
How long does a typical care plan last?
It depends entirely on your presentation and how your body responds to treatment.
Some patients see significant improvement in 4–6 weeks. Others need several months.
The care plan is built from what you actually report during treatment—not from a pre-determined billing calendar. If you're improving, the plan continues. If you're not improving, the plan changes.
The goal is to get you to a point where you don't need ongoing care—not to keep you coming back indefinitely because that's how the business model works.
The Real Question Isn't Which One Works—It's Which One Fits Your Case
If your disc problem is a mechanical breakdown that hasn't crossed into surgical emergency territory, you owe it to yourself to see if the system can be restored before you permanently alter it.
Surgery removes a symptom. It locks two vertebrae together because the disc between them failed. But it doesn't ask why the disc failed. It doesn't address the movement restriction, the postural breakdown, or the nervous system dysfunction that caused the disc to herniate in the first place.
Those problems are still there after surgery—you've just removed the segment that was showing the damage.
Non-invasive disc recovery asks why the disc failed and then works to correct the breakdown. It decompresses the nerve. It restores motion to the fixated segments. It retrains the muscles and nervous system to stabilize the area.
Not every case responds. But when it does, you've recovered function without surgically altering your spine's structure. And when it doesn't respond, you haven't lost anything—you've ruled out conservative care and moved forward with better information.
The surgical timeline doesn't disappear because you spent a few weeks trying a different approach. If conservative care isn't working, that becomes clear within 4–8 weeks, and you can proceed to surgery with the knowledge that you tried the non-invasive path first.
But if you go straight to surgery without ever addressing the root cause, you'll never know whether your body could've adapted on its own.
If you're dealing with nerve symptoms that radiate down your leg, if you've been told surgery is your only option, or if you're sitting with a surgical recommendation and no clear understanding of what else exists—that's worth one conversation.
If you're sitting in Morton, Peoria, or anywhere in central Illinois with a surgical recommendation in hand and you're not sure whether you've actually exhausted your conservative options, that assessment is the next step.
A chiropractic evaluation at Touch of Wellness Chiropractic starts with what you actually report—not a standard protocol applied to every disc case that walks through the door.
If your disc problem can be managed conservatively, you'll get a realistic care plan with measurable benchmarks. If it can't, you'll get an honest answer and an appropriate referral.
The goal isn't to avoid surgery at all costs. The goal is to determine whether your spine's mechanical breakdown can be corrected before you make a permanent structural change. If it can, you've recovered without surgery. If it can't, you've ruled out conservative care and moved forward with better information.
Find out what your assessment looks like.
If your disc has been dismissed as something you'll just have to live with, or if you've been told surgery is the only option without a clear explanation of why—that's worth investigating.
Not every case is fixable. But when the root cause gets addressed instead of just the symptom, recovery happens more often than most people expect.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet