
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
What Is the Biological Link Between Chronic Stress and Physical Misalignment?
Chronic stress physically changes spinal structure. That is not a metaphor — it is a measurable biological mechanism.
When the brain registers sustained stress, the autonomic nervous system shifts into sympathetic dominance. That shift shuts down the parasympathetic recovery cycles the musculoskeletal system needs to maintain joint balance. The body locks into a low-grade defensive state. The spine absorbs the structural consequence.
At the muscular level, psychological stress selectively activates postural motor units in slow-twitch fibers, pulling asymmetrically across individual vertebral segments. Surface electromyography research confirms that stress-driven activation increases resting muscle micro-tension in the upper trapezius by up to 35%. That is not soreness. That is sustained, asymmetric mechanical force applied to the vertebral column — during rest.
At the hormonal level, chronic HPA axis activation elevates cortisol. Sustained cortisol elevation inhibits collagen synthesis and progressively weakens spinal ligament integrity. Ligaments that lose tensile strength allow spinal segments to drift. The deviation is gradual. And it is measurable.
Clinical data confirms the connection. Sagittal spinal alignment parameters show a direct correlation between psychological distress levels and structural deviations — including forward head shift. The misalignment shows up on assessment.
The pain layer compounds everything. Prolonged stress lowers the mechanical activation threshold of spinal nociceptors through spinal hyperalgesia. Minor structural deviations that would otherwise register as mild discomfort get amplified into severe pain signals. The nervous system, already under load, magnifies what it detects.
The spine is downstream of the dial. Resolving stress-induced misalignment requires targeting the neurological loop — sympathetic dominance, altered motor firing, hormonal ligament degradation, pain amplification — as a system. Treating the vertebra that moved without addressing the signal driving it produces temporary improvement at best. The spine will keep responding to what the nervous system keeps sending.
Last Updated: June 22, 2026
- • Stress Is a Physical Event, Not Just a Mental One
- • Why the Cookie-Cutter Protocol Fails Stress-Driven Misalignment
- • How the Sympathetic Override Locks Your Spine in Place
- • The Measurable Structural Damage Chronic Stress Leaves Behind
- • Reading the Physical Signs Your Nervous System Is in Overload
-
• Frequently Asked Questions
- • Why does stress-related physical misalignment keep returning even after a standard massage?
- • How long does it typically take to retrain the nervous system out of a chronic stress-tension loop?
- • Why do cookie-cutter spinal adjustment protocols fail when dealing with chronic stress?
- • Can long-term physiological stress cause permanent structural changes in spinal alignment?
- • If my external stress sources cannot change, is it still possible to correct my physical alignment?
- • What It Actually Takes to Break the Stress-Misalignment Loop
Stress Is a Physical Event, Not Just a Mental One

You already know this feeling. The shoulders that won't drop. The neck that stays locked no matter what you do to it. That's not coincidence — and it's not in your head.
Here's the thing: stress isn't a light switch. It's a dial. It doesn't just shift your mood — it cranks the output of your entire autonomic nervous system. And your spine sits directly downstream of that signal. The higher the dial runs, the harder your musculoskeletal system works to hold a defensive position it was never designed to maintain long-term.
NIH-published electromyography research puts a number on it: psychological stress increases resting muscle micro-tension in the upper trapezius by up to 35%. That's not soreness from a hard workout. That is sustained mechanical force being applied to your vertebral column while you're sitting completely still — driven entirely by nervous system output, not by anything you did with your posture.
The Hormonal Cascade That Reaches Your Spine
But muscle tension is only the first layer. Stress reaches your spine through your hormones, too — and that path is slower, quieter, and far more destructive.
Chronic stress keeps the HPA axis — your body's central stress-response system — running at elevated output. That sustained activation drives cortisol up. And NIH research on HPA axis effects shows that chronically elevated cortisol actively inhibits collagen synthesis. Collagen is what keeps spinal ligaments strong and tensile. When synthesis slows, ligament integrity degrades. Spinal segments lose their structural hold and begin to drift.
So the pathway from stress to misalignment isn't abstract. It runs through measurable hormonal chemistry — the same chemistry that nervous system recovery in Morton targets clinically when the downstream structural damage is already visible on assessment. The cortisol load changes the tissue. Changed tissue allows structural drift. Structural drift shows up on the table.
Why Most People Never Connect the Two
Most people reach for a massage when stress locks up their back. Or better sleep. Or a standing desk. Those things help — for a few days. Then the tension comes back, and they're right where they started.
But the tension keeps coming back because the dial never moved. The biological driver is still running. The sympathetic nervous system is still telling your postural muscles to brace. The stress-related muscle tension people try to massage away is a downstream output. It is not the source. Treating it like the source is why nothing holds.
That's the gap. When the neurological signal goes unaddressed, the physical pain gets labeled as stress and the structural damage gets ignored entirely. That is exactly where individualized chiropractic care becomes the conversation most patients never had with any previous provider. Not because the pain wasn't real — but because no one ever connected what they were feeling in their body to what their nervous system was doing biologically.
| Stress Mechanism | Biological Action | Physical Target | Measurable Outcome |
|---|---|---|---|
| Sympathetic nervous system activation | Triggers sustained low-grade defensive bracing in postural muscles | Upper trapezius and cervical stabilizers | Up to 35% increase in resting muscle micro-tension |
| HPA axis cortisol elevation | Inhibits collagen synthesis, degrading the tensile strength of spinal ligaments | Spinal ligaments and connective tissue | Progressive loss of structural hold; spinal segments drift out of position |
Why the Cookie-Cutter Protocol Fails Stress-Driven Misalignment
The cookie-cutter protocol bets everything on one assumption: the vertebra moved on its own. Move it back, job done.
That assumption is wrong. And it's why the pain keeps coming back.
Here's what's actually happening. Chronic stress locks the autonomic nervous system into sympathetic dominance. The postural muscles respond by generating asymmetric traction across individual vertebral segments.
The vertebra isn't just sitting out of place. Something is actively pulling it there. And that signal is still running.
So when a provider adjusts that segment and sends you home, the signal doesn't turn off. The same motor unit firing pattern is still active. The same sympathetic override is still suppressing the parasympathetic recovery cycles your joints depend on.
The dial is still turned up. And within days — sometimes hours — the spine responds accordingly.
The Rejected Model: Adjust and Repeat
Here's what the rejected model looks like in practice. You come in with neck pain or a locked low back. The provider runs the same adjustment sequence they ran on the last fifteen patients. They find the segment that moved, move it back, and book you for next week.
No assessment of what's driving the pattern. No inquiry into whether signs of chronic nervous system overload are feeding the structural problem. Just the sequence.
That model works fine for acute mechanical injury. You fell, something shifted, you get it corrected, the body heals.
But stress-driven misalignment isn't a one-time mechanical event. It's a continuous neurological output. The spine is downstream of a dial that never got turned down.
Mental stress selectively fires postural motor units in slow-twitch muscle fibers. That firing creates asymmetric traction across vertebral segments — and a single adjustment session does nothing to that pattern.
The moment the nervous system reasserts its load, the firing restarts. Treating the structure without addressing the neurological driver isn't a conservative approach. It is the clinical definition of repeating what isn't working.
And yet that model is the industry default. Run the protocol. Collect the visit. Rebook.
The patient gets a week of relief, then slides back. The provider calls it a chronic condition requiring long-term maintenance. What it actually is — in many stress-driven cases — is a neurological loop that was never identified. Not once. Not by anyone.
Who This Approach Doesn't Work For
This approach doesn't work for the patient whose misalignment is sustained by a nervous system that hasn't had a parasympathetic recovery window in months. It doesn't work for the patient whose neck seizes every time a high-pressure work cycle hits.
And it doesn't work for the patient who has had the same vertebral segment adjusted dozens of times with the same temporary result. Same fix. Same regression. No one asking why.
But there's a specific reader this section is written for directly: the one who has already decided chiropractic care doesn't work before the assessment is finished.
That reader arrives with a closed verdict. They sit through the evaluation, nod along, then dismiss every clinical recommendation — because their GP called it pseudoscience, or because a previous provider ran the same adjustment sequence on them three times and it didn't hold. That prior experience is real. The conclusion drawn from it isn't necessarily.
If you need the provider to replicate a prior sequence before the findings are even reviewed — this isn't the right fit.
The clinical starting point here is always the assessment. Not the protocol. Not the previous provider's habits. If that's a problem before care begins, that's important information for both of us.
| Approach | What It Addresses | What It Ignores | Why Misalignment Returns |
|---|---|---|---|
| Cookie-Cutter Adjustment Protocol | The vertebral segment that moved out of position | The neurological signal actively pulling it back out of place | The same sympathetic override and asymmetric motor unit firing pattern restarts immediately after the session ends |
| Symptom-Only Pain Management | The reported pain level at the time of the visit | The autonomic nervous system load sustaining the pain signal | Parasympathetic recovery is still suppressed — the musculoskeletal system never enters a repair window |
| Standardized Visit-Count Maintenance Plan | Visit frequency and structural symptom recurrence | Whether stress-driven neurological patterning is feeding the structural problem | Misalignment is treated as a chronic structural condition when it is actually a continuous neurological output |
| Acute Mechanical Injury Model Applied to Stress Cases | The specific segment or region showing restriction or displacement | The postural motor unit activation pattern creating asymmetric vertebral traction | Without identifying the biological driver, correction is temporary — the spine responds to the signal the nervous system keeps sending |
How the Sympathetic Override Locks Your Spine in Place
The sympathetic nervous system is not the villain here. Spike, respond, recover — that's the design. But chronic stress removes the recovery half. What's left is sustained sympathetic dominance. And your spine lives inside the consequences of that, every single day.
That dominance isn't sitting still. It's actively suppressing the parasympathetic micro-recovery cycles your joints depend on — the biological window where micro-damage gets repaired and position gets maintained. The dial is turned up. The body never gets a chance to reset. Every structure downstream of that signal — postural muscles, spinal ligaments, vertebral segments — holds a position it was never designed to hold indefinitely.
So the spine doesn't drift out of alignment by accident. It gets pulled there by an active neurological output and held there by a system that's lost its off-switch. That's not a structural problem with a structural solution. That's a systems problem — and it requires a systems assessment.
Asymmetric Muscle Firing and What It Does to Vertebral Position
Here's the mechanism most providers skip entirely. Mental stress doesn't tighten muscles globally. It selectively activates postural motor units in low-threshold slow-twitch muscle fibers. Those fibers are built for endurance — they don't fatigue quickly. And when stress keeps triggering them asymmetrically, one side of the neck pulls harder than the other. One shoulder holds higher. One set of paraspinals braces more aggressively than the other.
That asymmetric firing generates uneven traction across individual vertebral segments. The vertebra doesn't move because something mechanical failed. It moves because one side of the muscular system is pulling harder — and that pull is being driven by cognitive load, not a bad lift or a car accident. The cause is neurological. The evidence shows up structurally.
That recurring neck tightness. The shoulder that won't drop. The low back that seizes every Monday. Patients describing stress-related muscle tension in those exact terms are usually reporting this pattern precisely. The asymmetric motor unit firing is already underway. Standard care addresses where the vertebra ended up. A systems assessment asks what neurological firing pattern put it there — and why it keeps putting it back.
Why Stress-Driven Pain Feels Worse Than It Should
Prolonged stress also lowers the mechanical activation threshold of the spine's pain receptors through spinal hyperalgesia. The receptors get sensitized. They fire at lower stimulus levels than they normally would. A minor structural deviation that would ordinarily register as mild discomfort gets amplified into a severe pain signal — not because more damage occurred, but because the nervous system's sensitivity got turned all the way up alongside everything else.
That's why stress-driven pain gets misread so often. The patient reports an eight out of ten. The imaging shows a two. The provider assumes the patient is exaggerating. But a chronically sensitized pain-detection system does exactly this — it magnifies what it detects. The pain is real. The biology producing it is the problem.
And this is where the dial metaphor earns its keep. If the nervous system is the dial — and sympathetic dominance is the dial turned all the way up — then pain sensitivity, motor unit firing, and structural position are all downstream outputs of the same control. Adjust the vertebra without turning down the dial, and every downstream output stays intact. The pain returns. The asymmetric pull restarts. The spine moves back. The patient gets labeled a chronic case, when what they actually have is an unaddressed neurological loop that nobody stopped to assess.
| Autonomic State | Muscle Behavior | Joint Effect | Pain Amplification |
|---|---|---|---|
| Sympathetic dominance (chronic stress state) | Parasympathetic micro-recovery cycles suppressed; postural muscles held in sustained contraction | Joints lose natural repair windows; vertebral segments held out of position by continuous muscular load | Baseline pain sensitivity elevated; minor deviations register as significant pain signals |
| Cognitive stress load (acute or chronic) | Low-threshold slow-twitch postural motor units fire asymmetrically in neck and shoulder muscles | Uneven traction generated across individual vertebral segments; one side pulls harder than the other | Structural deviation produced by neurological output, not mechanical injury — amplified by sensitized nociceptors |
| Prolonged sympathetic activation (chronic stress) | Postural muscles maintain defensive bracing patterns; slow-twitch fibers sustain asymmetric load without fatiguing | Vertebral segments held in deviation by enduring muscular traction; structural correction does not hold without neurological reset | Spinal hyperalgesia lowers mechanical pain threshold; minor misalignments amplified into severe pain signals |
The Measurable Structural Damage Chronic Stress Leaves Behind
The mechanism is the driver. But the driver leaves evidence.
Chronic stress doesn't just hold the spine in a bad position. It chemically degrades the structures that were supposed to hold it in the right one. That damage shows up on assessment. It shows up on imaging. It's not a subjective complaint — it's a clinical finding.
Here's the distinction that matters. A spine pulled out of position by asymmetric motor unit firing can be released — once the neurological driver is addressed. But when the ligaments supporting those segments have been weakened by months of cortisol exposure, the tissue itself is less capable of holding any correction.
The dial problem and the tissue problem compound each other. You don't get to solve one and call it done.
This is where stress stops being an emotional label and becomes a structural diagnosis.
The deviations are documentable. The damage is measurable. What patients feel in their body maps directly to what's happening in their nervous system — not as a metaphor, but as something that shows up on assessment.
Cortisol, Collagen, and the Weakening of Spinal Ligaments
Here's what most providers don't explain. When the HPA axis stays activated under chronic stress, cortisol levels don't spike and drop — they stay elevated. And one of cortisol's systemic effects is the suppression of collagen synthesis.
Collagen is the primary structural protein in spinal ligaments. Less collagen production means ligaments that are progressively less capable of maintaining joint integrity. The hormonal cascade isn't just making you feel tense — it's changing the tissue.
So the ligaments that are supposed to stabilize each vertebral segment are being chemically degraded by the same hormonal cascade that's also firing asymmetric muscle tension. The motor units pull the vertebra. The weakened ligaments offer less resistance. The structural deviation deepens.
That's not a mechanical problem with a mechanical solution. It's a systems failure. And you can't see it clearly without a systems lens.
Some patients weighing stress relief through medication against addressing the biological mechanisms directly are asking exactly the right question — they just need the complete answer.
Cortisol-driven collagen loss doesn't pause because the pain signal was chemically suppressed. The structural degradation continues regardless of whether the symptom gets quieted. Numbing the output doesn't turn down the dial.
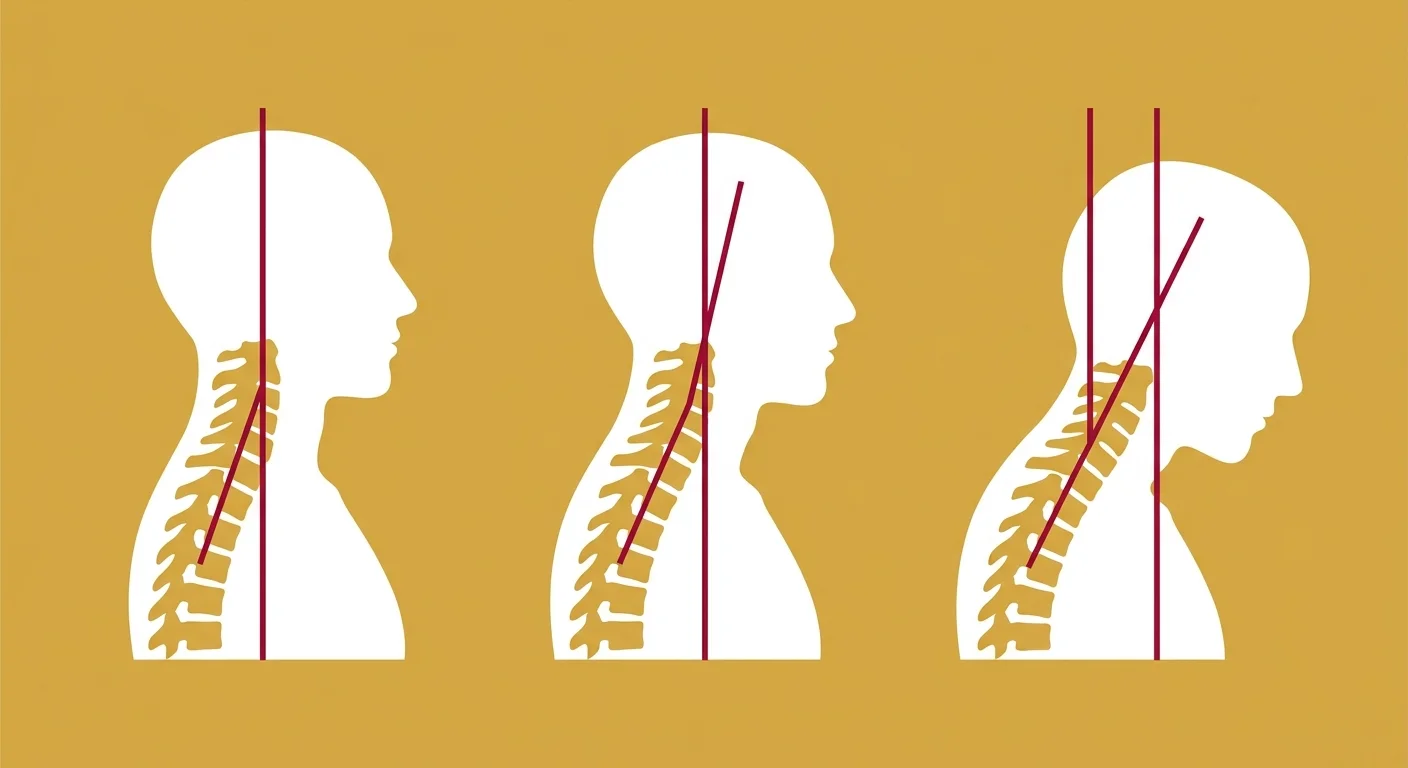
Forward Head Shift and the Sagittal Alignment Data
The structural evidence doesn't stay hidden. NIH clinical findings confirm that psychological distress correlates directly with measurable sagittal spinal alignment deviations — including forward head shift.
That's not a subjective complaint. It's a documentable postural change that corresponds to a documented stress load.
Forward head shift carries a specific mechanical consequence. For every inch the head migrates forward of its neutral position, the effective load on the cervical spine increases substantially.
And when that shift is being driven by chronic sympathetic activation — not by a single mechanical event — corrective approaches that ignore the neurological driver won't hold. The dial is still turned up. The head follows.
That's the clinical picture chronic stress leaves behind. A spine pulled into measurable structural deviation. Ligaments chemically less equipped to resist that pull. A pain system sensitized to amplify every minor deviation into a major signal.
The dial stayed turned up. The downstream evidence accumulated.
None of it resolves by moving the vertebra without addressing what moved it.
| Structural Marker | Stress Mechanism Responsible | Clinical Evidence | Reversibility |
|---|---|---|---|
| Spinal Ligament Integrity | Chronic HPA axis activation drives sustained cortisol elevation, which inhibits collagen synthesis — the primary structural protein in spinal ligaments | Cortisol elevation from sustained HPA axis activation inhibits systemic collagen synthesis and degrades spinal ligament stability | Partially reversible — ligament tissue can recover when cortisol load is reduced, but structural degradation accumulated over extended periods requires active rehabilitation, not passive correction |
| Sagittal Spinal Alignment | Psychological distress drives asymmetric motor unit firing and sustained postural muscle tension, producing measurable forward migration of the cervical spine | Clinical sagittal spinal alignment parameters confirm psychological distress correlates directly with measurable structural deviations, including forward head shift | Reversible when the neurological driver is addressed — postural deviation driven by active sympathetic output can be released; deviation compounded by ligament degradation requires a combined approach |
| Forward Head Shift | Chronic sympathetic dominance sustains the postural motor unit activation that migrates the head forward of its neutral cervical position | Psychological distress is directly correlated with forward head shift as a documentable sagittal deviation — not a subjective complaint | Reversible when the sympathetic loop driving the shift is interrupted — but standard corrective approaches that ignore the neurological driver predictably fail to hold the correction |
Reading the Physical Signs Your Nervous System Is in Overload

These mechanisms don't stay invisible. They surface. And they surface as patterns patients have been living with so long they stopped treating them as symptoms.
That's the clinical problem. By the time someone walks in, the adaptation is already complete. They stopped turning their head all the way to the left. They learned to sleep on one side. They figured out which movements to skip. The body built workarounds, and the workarounds became the new normal. Nobody flagged them as symptoms. They just became how that person moves through their day.
But those patterns aren't random. They map directly to what's building underneath, neurologically and structurally. Reading them as signals — not coincidences — is where the real assessment starts.
The Body Signals That Map to Sympathetic Dominance
Research using surface electromyography shows psychological stress increases resting muscle micro-tension in the upper trapezius by up to 35%. You feel that as the shoulder that won't drop. The neck that never fully releases between sessions. The jaw that's already clenched when you open your eyes in the morning. Those aren't posture problems you caused by sitting wrong. They're the physical output of a nervous system that hasn't found its off-switch — and they show up consistently, because the signal driving them never stopped.
And because the motor unit firing is asymmetric, the symptoms are asymmetric too. One shoulder sits higher. The right side of the neck braces while the left releases. The low back seizes on one side and not the other. Patients ask why the same side reloads every time. The answer is that the firing pattern was never touched. Only the structural result got treated. The dial stayed turned up, so the output restarted.
Here's the piece that confuses patients most. When spinal hyperalgesia is active, minor positional deviations produce pain signals that are way out of proportion to what's structurally there. So the patient reporting an eight out of ten — when imaging shows something mild — isn't exaggerating. Their nociceptors are firing at a lowered threshold. The problem isn't their perception. It's the sensitized system producing it. Everything downstream gets amplified. What should register as a manageable ache registers as severe.
When to Stop Waiting and Get Assessed
The threshold question isn't complicated. If the same symptoms keep returning after care — the correction holds for a week, then reloads, the shoulder drops on the table and climbs back by Thursday — the neurological driver hasn't been addressed. That pattern is the signal. It is not a chronic condition. It is an unresolved loop.
For patients dealing with persistent tension, asymmetric bracing, or pain that doesn't match the structural findings on imaging, the missing piece is a clinical picture that goes deeper than symptom management. Advanced Shockwave Therapy combined with a nervous system evaluation builds that picture — showing not just where the structure moved, but what's still pulling it. At Touch of Wellness Chiropractic, the assessment drives what comes next. That order doesn't reverse.
When the dial stays turned up, the body keeps producing the same outputs. The recurring tension. The asymmetric holding patterns. The pain that doesn't match the imaging. Those aren't separate problems to chip away at one at a time. They're the body reporting that the neurological loop is still running. The signs of chronic nervous system overload that have been building for months don't resolve by waiting. They resolve when the loop does.
Frequently Asked Questions
The biology is settled. The loop is real, measurable, and structural.
But knowing the mechanism doesn't answer the question you're actually sitting with: can anything change?
Here are the real questions. Answered without hedging.
Why does stress-related physical misalignment keep returning even after a standard massage?
Massage works on the output. The signal producing the tension is still running.
Psychological stress selectively fires postural motor units in the upper trapezius. Surface electromyography research confirms resting micro-tension in those muscles increases by up to 35% under psychological stress. When the sympathetic nervous system stays dominant, those muscles reload. Every time.
The correction doesn't hold because the driver was never interrupted. Massage releases what the loop just created. The loop keeps creating it.
How long does it typically take to retrain the nervous system out of a chronic stress-tension loop?
Any provider who quotes you a timeline before finishing an assessment is guessing. There is no universal number.
What the research does confirm: retraining requires parasympathetic recovery cycles to actually run. Those cycles shut down while sympathetic dominance holds. So the first clinical priority isn't spinal adjustment — it's reducing the neurological lock-in enough for the body's own repair to restart.
How long that takes depends on how entrenched the pattern is, how you respond, and whether the care plan changes when something isn't working. Expect a process. Not an event.
Why do cookie-cutter spinal adjustment protocols fail when dealing with chronic stress?
Because the protocol is built on one assumption: the vertebra moved, so move it back. That's the whole model.
But the vertebra didn't move on its own. Asymmetric motor unit firing pulled it there — driven by a sympathetic nervous system the protocol never assessed. Clinical sagittal alignment research confirms that spinal structural deviations correlate directly with psychological distress levels. A standard adjustment sequence that ignores that correlation produces a correction the nervous system immediately starts undoing.
The same side reloads because the same pattern is still running. That's not a chronic condition. That's an unaddressed loop.
Can long-term physiological stress cause permanent structural changes in spinal alignment?
Yes. Clinical research confirms that prolonged distress produces measurable, documentable structural deviations — including forward head shift — corresponding directly to sustained psychological stress levels.
And when spinal hyperalgesia is active, even minor positional shifts produce amplified pain signals. The structural changes don't need to be dramatic to be clinically significant.
Whether they're reversible depends on duration, severity, and whether care starts while structural integrity still exists to work with. Earlier is better. But the more important question isn't whether change is possible. It's whether your provider is looking at the right thing.
If my external stress sources cannot change, is it still possible to correct my physical alignment?
Yes. And this is where most people get stuck — they assume the stress source has to go away first. It doesn't.
Chronic sympathetic dominance shuts down the parasympathetic recovery cycles the body needs to maintain joint balance. Those cycles can be reactivated even when the stressor remains. When the nervous system's response to that load shifts — when the dial comes down even partway — the downstream outputs shift with it.
The muscle micro-tension that research measures at up to 35% above baseline begins to drop. The asymmetric pull reduces. The spine stops being held in the same compensated position.
The stressor doesn't have to disappear for the biological response to change. That's the clinical target.
What It Actually Takes to Break the Stress-Misalignment Loop
Every section here has been making the same argument from a different angle. The spine doesn't move on its own. It gets pulled — by asymmetric motor unit firing, by ligaments that cortisol has chemically degraded, by a pain system sensitized to turn minor deviations into something unbearable.
Moving the vertebra without addressing what moved it means treating the output while the control stays on.
That's why the same side reloads. That's why the correction holds for a week and then doesn't. The dial is still turned up. The spine keeps responding to what the nervous system keeps sending.
Breaking the loop means targeting it at the source. That requires a clinical lens that treats chronic stress as a biological mechanism — not an emotional label — and an assessment process built around what the patient actually reports, not what a standard protocol assumes.
Dr. Karen Hannah's Zoology background is exactly that lens. Whole-body biological systems analysis applied to a problem that is, at its core, a systems failure. Not a skeletal problem with a stress side effect. A systemic neurological lock-in with a skeletal consequence.
The sympathetic lock, the asymmetric pull, the structural degradation — none of it resolves in isolation. It resolves when the assessment goes upstream. When the neurological driver gets identified. When the work finally targets the control, not just the output.
So the question isn't whether chronic stress is affecting your spine. The research settled that.
The question is whether the provider assessing you is looking at the dial — or only at the vertebra. At Touch of Wellness Chiropractic, the assessment starts with the neurological picture. Because that's where the loop begins, and that's the only place it ends.
The spine is downstream of the dial. If no one has looked at the dial yet, the loop is still running.
The spine is downstream of the dial. If no one has assessed the dial yet, the loop is still running — and the same compensation pattern will keep pulling things back out of place. An assessment at Touch of Wellness Chiropractic starts with the neurological picture. Not the symptoms. Not a preset adjustment sequence. The actual pattern driving them.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet