
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
The biology of a chiropractic adjustment: What actually happens?
A chiropractic adjustment is a controlled, high-velocity force applied to a specific spinal joint. It restores normal motion and nervous system function. The audible pop is not bone cracking. It is tribonucleation — gas rapidly released from the joint's synovial fluid as pressure changes. Real-time MRI studies have visualized this event. The sound is created at joint separation, not from a bubble collapsing.
The mechanical event is only the beginning.
When a chiropractor delivers an adjustment, the controlled force stimulates sensory nerves called mechanoreceptors. These nerves send a volley of information to the central nervous system. This neurological input does not simply move the joint. It recalibrates how the brain and spinal cord process sensory information. It controls muscle tone. It coordinates movement. Research indicates spinal manipulation can reduce muscle strength deficits by 16% immediately following the intervention. Adjustments can also trigger an increase in beta-endorphins. These are neurochemicals that act as the body's natural painkillers. Studies measuring H-reflex and V-wave amplitudes show that spinal manipulation alters motor neuron excitability. It can influence spinal cord pathways.
The adjustment is not a mechanical fix for a symptom. It is a signal, not a switch. It is a precise neurological input to a biological system. The joint cavitation, the sensory flood, the neurochemical cascade that follows — all part of a systems response. The body does not interpret an adjustment as furniture moved back into place. It interprets it as new information. And it responds accordingly.
Last Updated: May 16, 2026
- • The Mechanical Event: What Creates the 'Pop'
- • The Neurological Input: How Mechanoreceptors Fire
- • The Systems Response: What Changes in the Body
- • Why the Cookie-Cutter Protocol Fails This Biology
-
• Frequently Asked Questions
- • What physically causes the 'popping' sound during a chiropractic adjustment?
- • How does an adjustment actually affect my nervous system's signals?
- • Are the biological effects of an adjustment temporary or do they create lasting changes?
- • What happens to the muscles and ligaments around the joint that is adjusted?
- • Can a single chiropractic adjustment really influence how my brain processes pain?
- • The Systems Biology Advantage
The Mechanical Event: What Creates the 'Pop'

The pop isn't the adjustment. It's a side effect.
Most people walk in expecting that sound. They've been conditioned to believe the noise means something worked. But the audible pop is just the Stage 1 Mechanical Event—the physical byproduct of controlled force applied to a restricted joint.
Here's what actually happens. When a chiropractor applies a high-velocity, low-amplitude thrust to a spinal segment, the joint surfaces separate rapidly. That separation drops the pressure inside the joint capsule. The synovial fluid — the lubricant that keeps joints moving smoothly — contains dissolved gases. When pressure drops, those gases come out of solution in a process called tribonucleation.
The sound you hear is the moment those gases form a bubble. Not the bubble popping. The bubble forming. That distinction matters, and for decades the research got it wrong.
The physics of tribonucleation
Tribonucleation is a pressure-driven phase change. Your joint's synovial fluid holds dissolved gases—carbon dioxide, nitrogen, a few others. When the joint surfaces separate fast enough, pressure inside the capsule drops. The gases can't stay dissolved anymore. They flash into gas phase.
That's the pop.
It's physics. Not magic. And it has nothing to do with whether the adjustment worked.
You can restore joint mobility without a sound. You can hear a pop and still have the same restricted motion two minutes later if the neurological input wasn't precise enough.
What real-time imaging reveals
For years, the assumption was that the sound came from a bubble collapsing.
Then researchers used real-time visualization of joint cavitation to watch it frame by frame. What they saw was the opposite.
The sound happens at the instant the joint separates and the cavity forms. The bubble doesn't disappear — it persists for a fraction of a second after the noise. That flipped decades of assumptions. The pop is the opening, not the closing. It's the pressure drop, not the collapse.
| Event | What Happens Physically | Why It Matters |
|---|---|---|
| Joint separation | Chiropractor applies controlled thrust; joint surfaces move apart rapidly, creating space inside the capsule | The separation is what drops pressure—without it, no gas release occurs |
| Pressure drop inside joint capsule | As surfaces separate, internal pressure falls below the threshold needed to keep gases dissolved in synovial fluid | This is the trigger for tribonucleation—the phase change from liquid to gas |
| Gas bubble formation (tribonucleation) | Dissolved gases flash into gas phase instantaneously, forming a visible cavity inside the joint | The audible pop occurs at this exact moment—not when the bubble collapses |
| Cavity persists briefly | The gas-filled space remains visible for a fraction of a second after the sound, then gradually reabsorbs | Real-time imaging proved the bubble doesn't pop—it forms, lingers, then dissolves |
| Joint motion restored | The separation resets the joint's position and range, allowing freer movement of the vertebral segment | This is the mechanical outcome—but the neurological cascade hasn't started yet |
The Neurological Input: How Mechanoreceptors Fire
The pop is just the starting gun.
The real event is the sensory volley it triggers in the nervous system.
The mechanical force of the adjustment doesn't just move bone. It compresses and stretches the soft tissue around the joint — ligaments, joint capsules, muscle spindles, and tendon organs. All of that tissue is loaded with sensory nerves called mechanoreceptors.
These are the body's motion detectors. They fire the instant they sense pressure, stretch, or movement.
When the adjustment happens, those receptors fire all at once. That's Stage 2 Neurological Input. A flood of proprioceptive data — information about joint position, movement speed, and tissue tension — gets transmitted up the spinal cord to the brain.
That's the signal the body actually responds to. Not the pop. The data.
What the adjustment actually stimulates
So where do these mechanoreceptors actually sit?
Everywhere. Ligaments stabilizing the vertebrae. The joint capsule wrapping the facet joint. Muscle spindles embedded in the paraspinal muscles. Golgi tendon organs at the muscle-tendon junction.
Every structure around the spine is wired with sensory nerve endings tuned to detect mechanical deformation. The adjustment hits all of them at once.
The adjustment doesn't turn pain off like flipping a switch. It changes the signal. A spinal adjustment stimulates sensory nerves called mechanoreceptors, sending a volley of information to the central nervous system. That sensory input competes with pain signals for bandwidth in the spinal cord.
More mechanoreceptor activity means less pain signal gets through. That's not theoretical. That's neurophysiological effects of spinal manipulation documented at the cellular level.
Where the information travels in the CNS
The sensory volley doesn't stop at the spinal cord. It travels up to the thalamus, the somatosensory cortex, the cerebellum, and the prefrontal cortex.
Each region processes a different dimension. Position. Movement. Coordination. Attention.
This is where the systems biology lens matters. The adjustment isn't resetting one joint. It's recalibrating how the human nervous system acts as the body's master controller.
The brain integrates the new data, updates its internal map of body position, and adjusts motor output accordingly. Muscle tone changes. Movement patterns shift. Pain thresholds recalibrate.
That's Stage 3 Systems Response. And it all starts with mechanoreceptors firing in the milliseconds after the joint separates.
| Receptor Type | What It Detects | Where the Signal Goes |
|---|---|---|
| Ligament Mechanoreceptors | Stretch, tension, and joint position at rest and during movement | Spinal cord dorsal horn, then thalamus and somatosensory cortex for position awareness |
| Joint Capsule Mechanoreceptors | Pressure changes and rapid deformation when the joint separates or compresses | Central nervous system via fast-conducting nerve fibers, influencing reflexive motor adjustments |
| Muscle Spindles | Changes in muscle length and the rate at which the muscle is being stretched | Spinal cord for reflex arcs, cerebellum for coordination, and motor cortex for movement planning |
| Golgi Tendon Organs | Tension at the muscle-tendon junction, signaling how much force the muscle is generating | Spinal cord to inhibit excessive muscle contraction, preventing tissue damage and regulating tone |
| Free Nerve Endings (Nociceptors) | Chemical irritation, inflammation, and tissue damage signals interpreted as pain | Spinal cord dorsal horn where mechanoreceptor input can gate pain transmission to the brain |
The Systems Response: What Changes in the Body
This is Stage 3 Systems Response. The adjustment stops being mechanical. It becomes functional.
The neural signal doesn't just reach the brain. It alters how the brain processes movement, pain, and coordination. Motor control improves. Pain thresholds shift. Spinal reflex pathways recalibrate.
That's not placebo. That's neuroscience.
And these changes happen immediately. Not over weeks. Not after a dozen visits. Within minutes.
The brain integrates the new proprioceptive data. It updates its internal map of the body. Motor output adjusts. Muscle tone changes. Movement patterns that were compensating for restricted motion start to normalize.
Pain signals flooding the nervous system get turned down.
This is the part most chiropractic offices never explain. They focus on the pop. They tell you the joint was out of place and now it's back in.
That's not systems biology. That's furniture repair.
The adjustment works because it recalibrates the nervous system — the body's master controller. Not because it shoved a bone back where it belongs.
Motor control and muscle function improvements
Research shows spinal manipulation can reduce muscle strength deficits by 16% immediately following the intervention. That's not a subjective improvement in how you feel. That's a measurable increase in force production. Documented through dynamometry and electromyography.
The adjustment changes corticospinal excitability. That's the efficiency with which the brain sends motor commands down the spinal cord to the muscles. More signal gets through. The muscle fires harder.
Here's why that matters. Chronic pain doesn't just hurt. It weakens. The nervous system starts inhibiting muscle activation to protect the area. You lose strength not because the muscle is damaged, but because the brain won't let it fire at full capacity.
The adjustment removes that inhibition. The sensory input from the mechanoreceptors tells the brain the joint is moving normally again. The motor system responds by increasing activation. Studies documenting changes in sensorimotor integration show this recalibration happening in real time.
Pain modulation through endorphin release
The adjustment also triggers an increase in beta-endorphins. These are neurochemicals that act as the body's natural painkillers. Beta-endorphins bind to opioid receptors in the brain and spinal cord. They produce hypoalgesic effects — a measurable reduction in pain perception.
This isn't masking symptoms. It's changing the neurochemical environment that processes pain signals.
The endorphin release isn't random. It's a direct response to the sensory input from the adjustment. The mechanoreceptor activation triggers a cascade that includes increased plasma beta-endorphin levels.
That's why patients often report feeling better immediately. Even before inflammation has time to resolve. The nervous system isn't waiting for tissue healing to catch up.
It's responding to new information right now.
Spinal reflex pathway recalibration
Studies measuring H-reflex and V-wave amplitudes show that spinal manipulation alters motor neuron excitability and can influence spinal cord pathways. The H-reflex is a measure of how easily a reflex arc fires in response to a stimulus. The V-wave measures voluntary motor drive from the brain to the muscle.
Both change after an adjustment. That means the adjustment isn't just affecting the joint. It's modulating the spinal cord circuits that control movement.
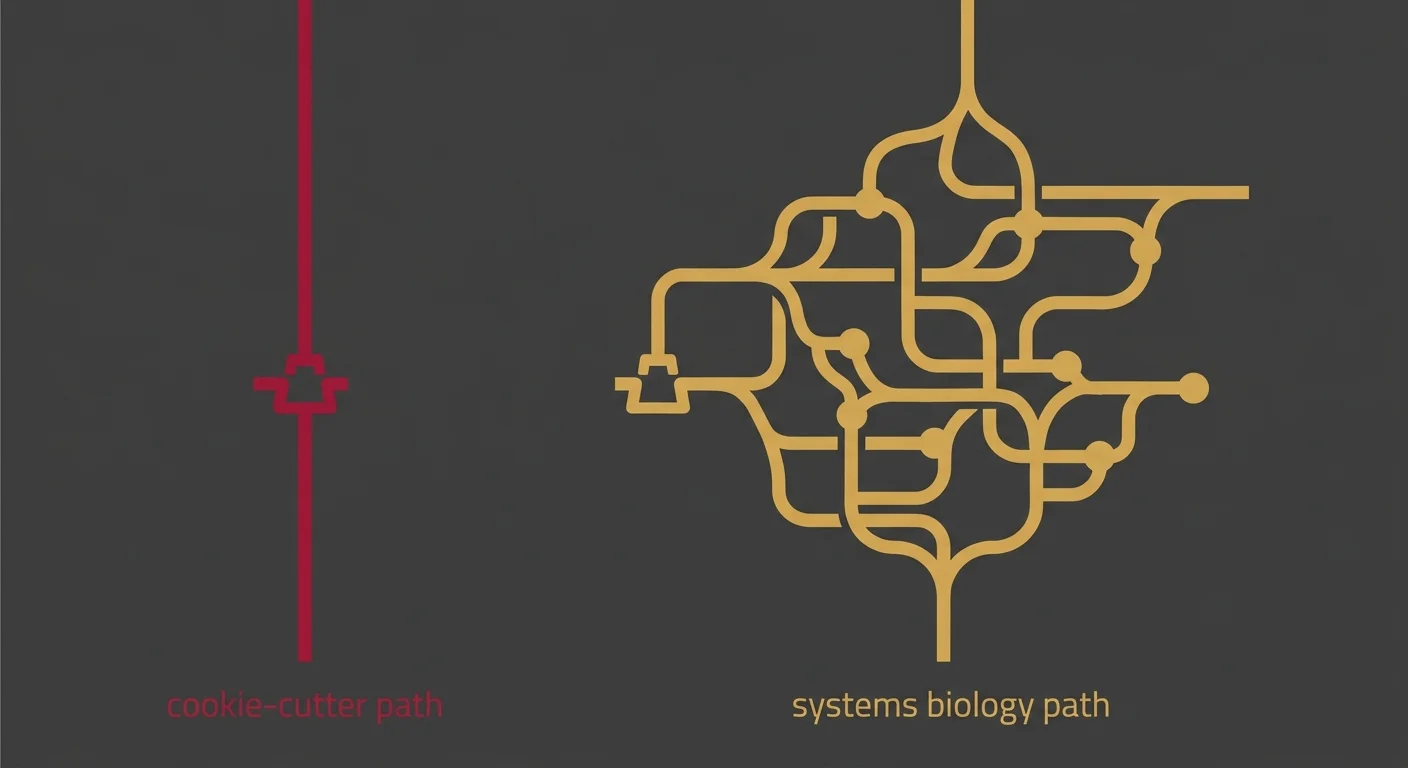
This is where the systems biology lens separates root-cause chiropractic care from the cookie-cutter model.
If you're just chasing the pop, you're treating the joint. If you're recalibrating spinal reflex pathways, you're treating the system. The adjustment is the input. The nervous system is the target.
And the changes documented in H-reflex and V-wave amplitudes prove the body responds at the level of motor neuron excitability, not just joint mobility. Practices that don't understand this distinction can alter motor neuron excitability by accident.
Dr. Karen does it by design.
| Biological System | Measured Change | Clinical Outcome |
|---|---|---|
| Motor Control System | 16% increase in muscle force production immediately post-adjustment | Reduced muscle inhibition, restored strength output, normalized movement patterns |
| Brain-to-Muscle Pathway | Changes in corticospinal excitability | Faster motor commands, improved coordination, reduced compensatory firing |
| Neurochemical System | Increased plasma beta-endorphin levels | Hypoalgesic effect, reduced pain perception without masking symptoms |
| Spinal Reflex Pathways | H-reflex amplitude changes | Altered motor neuron excitability, recalibrated reflex arc sensitivity |
| Voluntary Motor Drive | V-wave amplitude changes | Improved voluntary muscle activation, enhanced brain-to-muscle signal efficiency |
| Neurochemical | Mechanism | Effect on Pain Perception |
|---|---|---|
| Beta-Endorphins | Released in response to mechanoreceptor activation during the adjustment; bind to opioid receptors in the brain and spinal cord | Produce hypoalgesic effects—measurable reduction in pain perception without masking underlying dysfunction |
Why the Cookie-Cutter Protocol Fails This Biology
Most chiropractic offices treat the pop as the outcome. They're missing the entire neurological cascade.
Same adjustment sequence on every patient. Walk in with nerve pain, walk in with a headache, walk in with sciatica — you get the same protocol. When it doesn't work, they run it again.
That's not a care plan. That's a template.
The cookie-cutter protocol ignores mechanoreceptor stimulation, sensorimotor integration, and motor neuron excitability. It treats the adjustment as a mechanical fix instead of a neurological input.
The adjustment is the signal, not the switch.
But if you're just hunting for the pop, you're treating furniture.
The adjustment doesn't fail. The protocol was never matched to the patient's neurological presentation.
You can't recalibrate a system you haven't assessed.
Dr. Karen Hannah's whole-body biological systems analysis is built to avoid that failure. If the protocol doesn't change when the patient's response changes, you're not doing chiropractic care. You're doing repetition.
When the pop becomes the goal instead of the signal
When the pop becomes the goal, the adjustment turns into performance instead of treatment. The practitioner chases the sound. The patient expects the sound. And everyone forgets the sound has zero correlation with whether the central nervous system received the input it needed.
A spinal adjustment stimulates sensory nerves called mechanoreceptors. That's the event that matters.
The pop is just physics. Tribonucleation. Gas release. Joint separation. It's the acoustic byproduct of the pressure change. It doesn't tell you whether the mechanoreceptors fired. It doesn't tell you whether the sensorimotor cortex integrated the signal. It doesn't tell you whether motor control improved.
Research shows spinal manipulation can reduce muscle strength deficits by 16% right after the adjustment. That's the outcome. Not the sound.
The strength change happens because the adjustment recalibrated corticospinal excitability — the brain's ability to send motor commands to the muscles. You can get that result with or without the pop.
But if your entire clinical model is built around chasing the acoustic event, you're treating the wrong target.
What gets missed without a systems biology lens
The systems biology lens sees the adjustment as an input to a feedback loop. Mechanoreceptors fire. The spinal cord processes the signal. The brain integrates the data. Motor output changes. Pain thresholds shift. Muscle activation patterns normalize.
That's a cascade, not a single event.
Practices without that lens stop at Stage 1 — the Mechanical Event. They adjust the joint, hear the pop, and move on. They never assess whether the Neurological Input reached the central nervous system. They never verify whether the Systems Response happened.
If the patient still hurts two weeks later, they run the same protocol again and call it a flare-up.
This is why questions to ask your chiropractor about nervous system health matter more than questions about technique. The technique is the tool. The nervous system is the target.
If your chiropractor can't explain how the adjustment affects mechanoreceptor stimulation, sensorimotor integration, and motor control recalibration, they're treating joints. Not systems.
And if they can't explain what changes when the initial protocol doesn't produce results, they're repeating a script instead of doing biology. Unexplained does not mean untreatable. It means no one's looked at the right system yet.
Frequently Asked Questions
The biology is complex. So here's what patients ask once they realize an adjustment isn't just a pop.
These aren't abstract. They're the specific mechanisms that separate systems biology from symptom chasing. If your chiropractor can't answer them, that tells you everything about their clinical model.
What physically causes the 'popping' sound during a chiropractic adjustment?
The pop is tribonucleation. Gas released from synovial fluid. Pressure changes in the joint create a rapid shift. Gas bubbles form and release. That's the sound.
It's physics, not healing.
The adjustment doesn't require the pop to work. The pop doesn't confirm the adjustment worked. Real-time MRI studies show the sound happens at joint separation — an acoustic byproduct, not a clinical outcome.
How does an adjustment actually affect my nervous system's signals?
The adjustment stimulates mechanoreceptors — sensory nerves embedded in joint capsules. Those receptors fire when the joint moves. They send signals to your spinal cord and brain.
That's the Neurological Input stage.
Your central nervous system processes the data. Motor pathways adjust. Reflex thresholds shift. Pain processing changes. The adjustment is information. Your nervous system is the receiver. The pop is just noise in the background.
Are the biological effects of an adjustment temporary or do they create lasting changes?
Both.
The immediate effects are real and measurable. Beta-endorphin release happens right after the adjustment. That's temporary. But the sensorimotor integration changes can persist if reinforced. Motor neuron excitability shifts can stabilize with repeated input.
The nervous system is plastic — it learns. One adjustment sends a signal. A care plan teaches the system a new baseline. Temporary effects become lasting when the system gets enough input to rewire.
What happens to the muscles and ligaments around the joint that is adjusted?
Muscles respond to motor neuron signals. When the adjustment alters motor neuron excitability, muscle activation patterns change. Tight muscles can relax. Weak muscles can activate.
Ligaments don't contract or relax — they stabilize. But they respond to improved joint mechanics.
The adjustment recalibrates the nervous system's control over those tissues. It's not stretching the ligament. It's changing the motor command that governs the muscle pulling on it.
Can a single chiropractic adjustment really influence how my brain processes pain?
Yes.
Studies show adjustments trigger beta-endorphin release — natural painkillers. Beta-endorphins bind to opioid receptors in your brain. Pain thresholds shift immediately. That's not placebo. It's neurochemistry.
The adjustment also changes how your brain integrates sensory input. Sensorimotor cortex activity shifts after spinal manipulation. One adjustment changes how pain signals are processed. Multiple adjustments can retrain the brain's default pain response.
The Systems Biology Advantage
Once you understand this cascade, you can't unsee it.
The adjustment isn't magic. It's biology.
A controlled mechanical input that triggers a neurophysiological cascade across three distinct stages—the Mechanical Event, the Neurological Input, and the Systems Response. Most practices stop after Stage 1. They deliver the pop and call it done.
That's mechanical thinking applied to a living system. Not systems biology.
The adjustment is a signal, not a switch. Most chiropractors never learned the difference.
About Dr. Karen Hannah, DC: her clinical lens is built on a cross-species neurological framework. After witnessing a paralyzed kitten recover complete motor function in four days through spinal recalibration, she recognized that an adjustment is a precise signal to a live operating system, not just a mechanical movement.
She doesn't chase the pop. She recalibrates the nervous system.
The adjustment is the signal, not a switch. And when the initial protocol doesn't produce the Systems Response, she changes it. Not repeats it.
This isn't about friendly staff or cutting-edge equipment. It's a clinical assessment that drives the care plan, not a billing calendar. The mechanoreceptor input, the sensorimotor integration, and the motor control recalibration are all part of one cascade. And she treats them as such.
If your current provider can't explain how the adjustment affects your nervous system—not just your joints—that's important information.
If they run the same protocol on every patient regardless of response, that's not individualized care. That's a script.
The nervous system runs everything. When it's disrupted, nothing works right. And when a provider understands how to recalibrate it through precise neurological input, everything else starts working better too.
The systems biology advantage isn't theoretical. It's measurable. Documented. Reproducible.
The question isn't whether the adjustment works. The question is whether your chiropractor understands why it works—and what to do when it doesn't.
If you've been dismissed, handed a protocol that didn't change when your symptoms didn't either, or told the pop means it worked — you've seen the other model. Touch of Wellness Chiropractic doesn't chase the pop. Dr. Karen recalibrates the system. The adjustment is the signal, not a switch. And when it doesn't produce the response your nervous system needs, the plan changes. Not repeats. Your pain has been explained away long enough. If it's affecting your work, your sleep, or how you move through the day — that's past the threshold of waiting it out. Book an assessment.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet