
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
Non-Invasive Disc Recovery vs. Physical Therapy: Why One Fails Where The Other Succeeds
Physical therapy strengthens the muscles around the disc. It doesn't fix the disc. That's not a weakness of PT — it's a category error. You're building the container while the contents are still broken. Physical therapists typically prescribe exercises that target the abdominal muscles, back extensors, and hip stabilizers, working on the assumption that a stronger core will alleviate disc-related pain.
Non-invasive disc recovery, such as spinal decompression therapy, takes a fundamentally different approach. Instead of strengthening the muscles around the disc, it directly targets the disc itself. This method works by applying gentle, computer-controlled traction to the spine, creating negative pressure within the intervertebral disc space. This negative pressure retracts herniated disc material away from compressed nerve roots. That's the mechanism. Not theoretical — mechanical. More importantly, it creates a vacuum effect that draws in oxygen, nutrients, and healing fluids that the disc needs to repair itself. The disc is avascular, meaning it has no direct blood supply, so this pressure gradient is one of the few ways to promote actual healing of the disc tissue.
The fundamental difference is this: physical therapy addresses the mechanical support system around the disc by strengthening muscles. Non-invasive disc recovery addresses the mechanical pressure problem inside the disc itself. Physical therapy works on the container. Disc recovery works on the contents. When a disc is herniated or bulging, the nucleus pulposus has pushed through or against the outer annular fibers, creating pressure on surrounding nerve tissue. No amount of core strength can reverse that outward pressure or retract that material. Muscular support can prevent further injury and provide stability, but it cannot decompress an already-compromised disc or change the intradiscal pressure dynamics that are causing nerve compression and pain.
Physical therapy works for muscle strains. It works for postural dysfunction. When the problem is a herniated disc compressing a nerve, strengthening exercises don't resolve it. They manage it. That's the difference. The disc remains compromised, and the pain returns once the temporary relief from reduced activity or inflammation management wears off.
Last Updated: April 30, 2026
Why Physical Therapy Fails Most Disc Injuries
Most people walk into a PT office with disc pain and get handed the same protocol. Planks. Bird dogs. Bridges. A print-out with exercises they're supposed to do three times a week.
The assumption is simple: if you strengthen the core, the pain will go away.
And for a few weeks, it might. The inflammation settles. You feel stable. Then you go back to normal activity and the pain comes screaming back — because the disc itself never changed.
That's the cookie-cutter protocol problem. PT treats every disc case like a muscle weakness issue. And when it doesn't work after six weeks, you're told to keep doing the exercises. Same protocol. Same outcome.
The Cookie-Cutter Protocol Problem
Physical therapy protocols are built around one central assumption: that a disc injury is fundamentally a stability problem.
If the muscles around the spine are weak, the disc gets overloaded. Strengthen the muscles, reduce the load, problem solved.
Except that's not how disc injuries work.
According to Mayo Clinic, spinal decompression therapy works by creating negative pressure within the disc — something that core exercises physically cannot do. The disc is under pressure from the inside out. You can build the strongest core in the world, and it won't change what's happening inside that disc space.
But standard PT protocols don't account for that. They apply the same sequence to every patient — regardless of whether the disc is bulging, herniated, or fully ruptured. Regardless of whether nerve compression is present. Regardless of how the patient responds after the first month.
That's not care. That's a template. And when a template doesn't work, the answer isn't to repeat it louder.
Why Core Strength Alone Cannot Fix a Disc
Your core muscles support your spine. That's their job.
They stabilize movement, prevent excessive rotation, and take load off the discs during bending and lifting. If you have a weak core and you injure a disc, strengthening those muscles absolutely matters.
But core strength alone cannot fix a lumbar disc that's already herniated.
Here's why: the disc is a closed hydraulic system. When the nucleus pulposus breaks through the outer annular fibers and pushes against a nerve root, the only way to retract that material is to change the pressure inside the disc.
Core muscles sit outside that system. They can reduce the forces acting on the disc during movement, but they can't reverse the herniation. They can't pull the bulging material back in.
That requires negative intradiscal pressure — and that's where root-cause chiropractic care comes in.
| Function | Core Strength Impact | Disc Recovery Impact |
|---|---|---|
| Stabilize spine during movement | Yes — reduces excessive motion and load during activity | Indirect support — spinal stability helps maintain decompression results |
| Prevent future disc injury | Yes — stronger stabilizers reduce risk of new herniation | Indirect prevention — healed disc is less vulnerable when combined with stability |
| Retract herniated disc material | No — muscles cannot create intradiscal negative pressure | Yes — decompression creates vacuum effect that retracts bulging nucleus pulposus |
| Decompress nerve roots | No — nerve compression remains if disc bulge is unchanged | Yes — negative pressure reduces disc bulge and relieves nerve impingement |
| Restore nutrient flow to disc | No — core exercises do not change intradiscal fluid dynamics | Yes — pressure gradient draws healing nutrients into avascular disc tissue |
The Symptom Management Trap
Physical therapy does reduce pain — temporarily.
It improves flexibility. It teaches you how to move without aggravating the injury. It manages the symptoms.
But managing symptoms is not the same thing as resolving the cause.
Research published in The Spine Journal outlines the standard goals of PT for low back pain: reduce inflammation, improve range of motion, strengthen supporting musculature, and educate the patient on body mechanics. All valuable. All necessary for long-term spinal health.
None of them fix the disc.
So what happens? You finish your PT program. You feel better for a while. Then you lift something the wrong way, or you sit too long, or you twist getting out of the car — and the pain comes back.
Because the disc is still compromised. The intradiscal pressure problem was never addressed.
That's the trap. Symptom management keeps you functional. It doesn't make you whole.
The Mechanical Reality of Disc Injuries
If you want to understand why PT fails most disc injuries, you have to understand what's actually happening inside the disc.
Not the narrative. Not the theory. The mechanics.
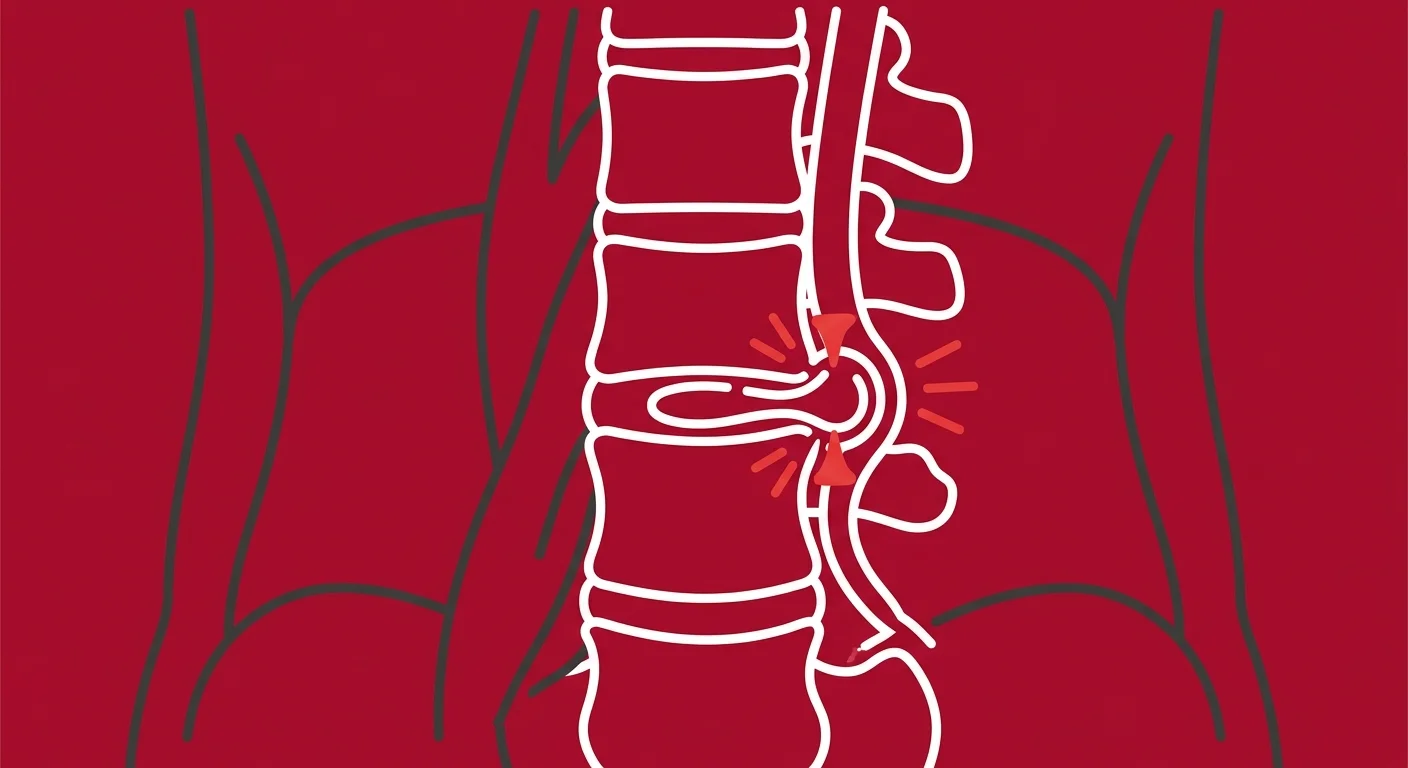
What Actually Happens Inside a Herniated Disc
Your intervertebral discs are shock absorbers.
Each one sits between two vertebrae and cushions the spine during movement. The outer layer — the annulus fibrosus — is made of tough, fibrous rings. The inner core — the nucleus pulposus — is a gel-like substance that distributes pressure across the disc.
When a disc herniates, the nucleus pulposus breaks through the annular fibers and pushes outward. If it pushes far enough, it compresses a spinal nerve root. That compression triggers inflammation, which irritates the nerve even further. The result is radiating pain, numbness, tingling, or weakness down the leg — classic sciatica symptoms.
According to Johns Hopkins Medicine, this process is often the result of age-related degeneration, but it can also occur from acute trauma or repetitive strain. Once the disc material is displaced, the body's natural healing mechanisms are limited — because the disc has no direct blood supply. It relies entirely on passive diffusion of nutrients from surrounding tissue.
That's the first mechanical problem PT can't solve. You can't exercise your way into better nutrient flow to an avascular disc. You need to change the pressure gradient.
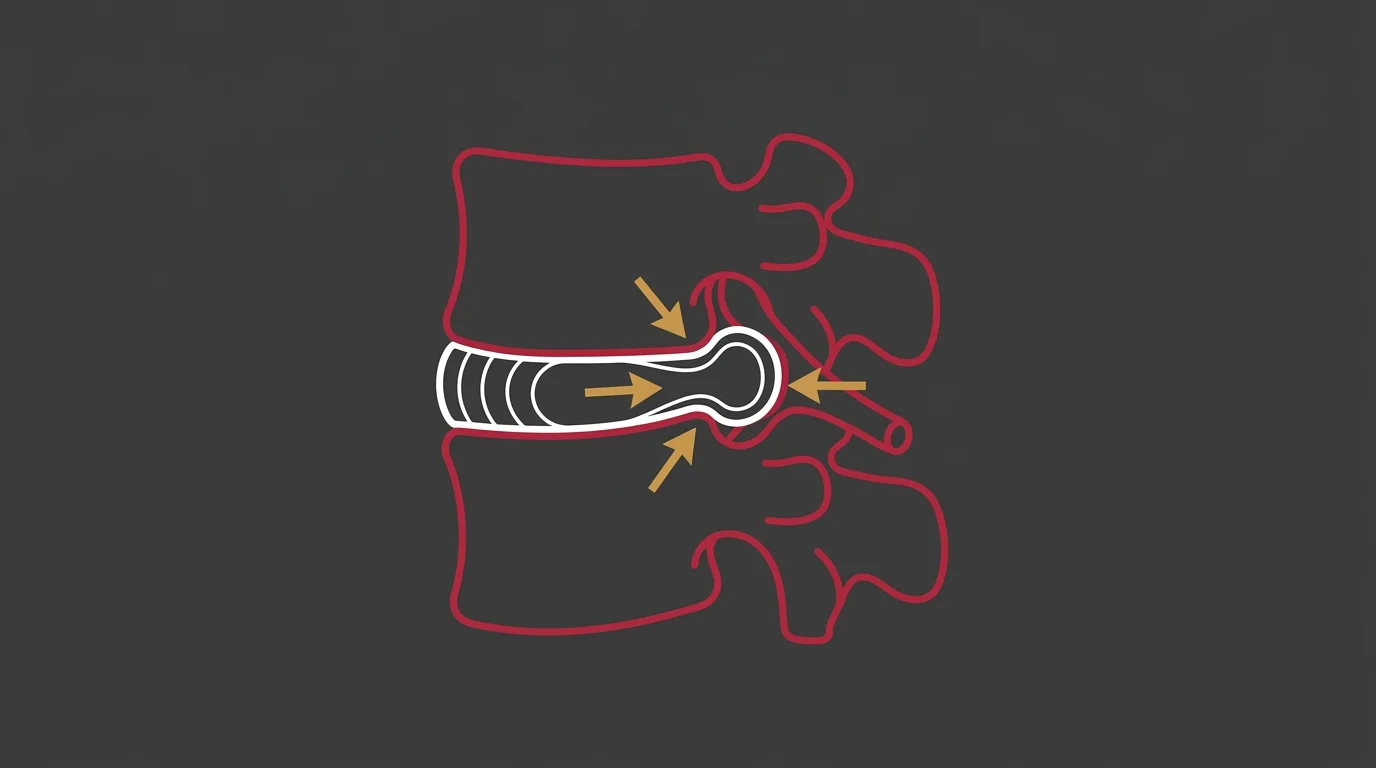
The Pressure Problem PT Cannot Solve
Here's the part most patients never get explained: a herniated disc is under constant outward pressure.
The nucleus pulposus is being pushed against the weakened annular wall by the mechanical load of your body weight, spinal curvature, and daily movement.
Physical therapy can reduce some of that load by improving your posture and strengthening your stabilizers. But it can't reverse the direction of that pressure. It can't pull the herniated material back into the disc space.
You're dealing with chronic or recurring pain because the mechanical cause is still active. The disc is still bulging. The nerve is still compressed.
Strengthening the muscles around that problem doesn't make the problem go away — it just makes you better at living with it.
And for some people, that's enough. But if you're reading this, it probably isn't.
| Problem | Cause | PT Target | Disc Recovery Target |
|---|---|---|---|
| Herniated disc material compressing nerve root | Nucleus pulposus breakthrough of annular fibers due to mechanical overload or degeneration | Strengthen core and back muscles to reduce spinal load and prevent further injury | Create negative intradiscal pressure to retract herniated material away from nerve |
| Radiating leg pain and numbness | Direct nerve compression plus inflammatory response | Reduce inflammation with rest, stretching, and activity modification | Decompress nerve root by reducing disc bulge and restoring normal spacing |
| Chronic recurring pain after initial improvement | Disc remains compromised; pressure dynamics unchanged | Maintain muscular support to manage symptoms long-term | Restore intradiscal pressure balance to promote actual disc healing |
| Limited nutrient flow to injured disc | Avascular disc tissue relies on passive diffusion, which is impaired when disc is compressed | No direct mechanism to improve nutrient delivery | Negative pressure gradient draws oxygen and healing nutrients into disc space |
What Non-Invasive Disc Recovery Actually Does
Non-invasive disc recovery doesn't strengthen the container.
It changes what's inside the container.
That's the fundamental difference. And that's why it works when PT doesn't.
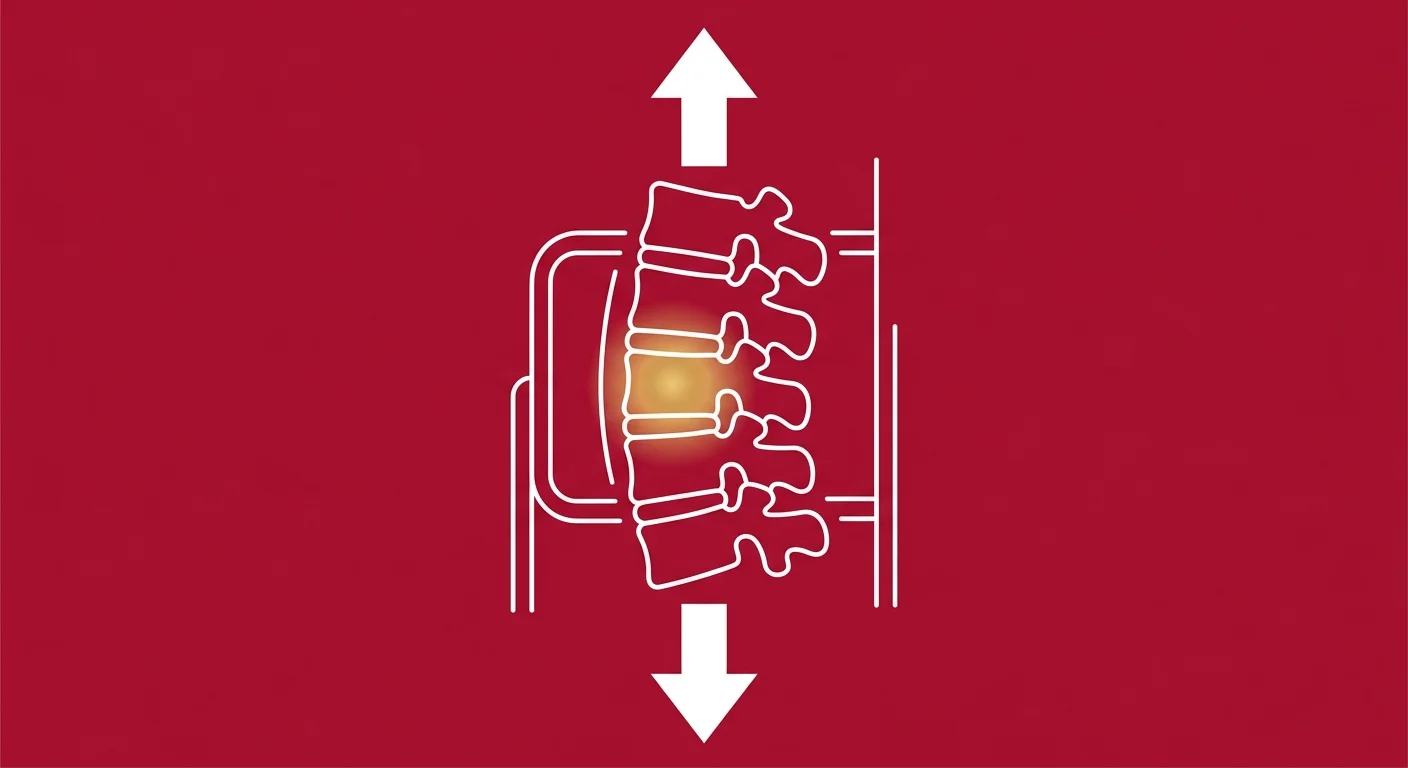
How Spinal Decompression Creates Negative Pressure
Spinal decompression therapy uses computer-controlled traction to gently stretch the spine in a very specific way.
The goal isn't just to pull the vertebrae apart — it's to create negative pressure inside the disc space.
When the spine is stretched with precise tension, the pressure inside the disc drops below atmospheric pressure. That creates a vacuum effect. The herniated disc material — which was being pushed outward by positive pressure — now experiences a reversal of force. The negative pressure helps retract the bulging nucleus pulposus back toward the center of the disc.
At the same time, that vacuum draws in oxygen, nutrients, and healing fluids that the disc desperately needs. Remember: the disc has no blood supply. It relies entirely on diffusion. Negative pressure is one of the few mechanisms that can actively promote nutrient flow into the disc tissue.
This is how non-invasive disc recovery works without back surgery. You're not cutting anything out. You're not fusing anything. You're creating the mechanical conditions the disc needs to heal itself.
A clinical study published in the National Library of Medicine examined the management of lumbar disc herniation with both chiropractic care and physical therapy. The study found that while both approaches had value, spinal decompression therapy offered a distinct mechanical advantage in cases where intradiscal pressure was the primary driver of symptoms.
The Healing Process
Here's what happens over the course of a decompression care plan:
In the first few weeks, most patients experience a reduction in nerve-related symptoms. The disc material retracts slightly. The nerve compression eases. Inflammation starts to settle.
This is the acute relief phase — and it's where a lot of people think they're done.
They're not.
The middle phase of care is where the disc actually begins to heal. The repeated negative pressure cycles encourage nutrient flow. The annular fibers start to repair. The disc regains some of its height and structural integrity.
This is the phase where patients often feel like they're back to normal — until they test it too hard and realize they're only 70% healed.
The final phase locks in the results. The disc stabilizes. The nerve pathways that were irritated for months finally calm down. The body adapts to the restored disc function.
And the care plan ends — not because a predetermined timeline ran out, but because the clinical markers say you're done.
That's how chiropractic care restores nervous system function. You're not managing the pain. You're resolving the mechanism that caused it.
Why This Is Not Simple Traction
People hear "spinal decompression" and think it's just a fancy inversion table.
It's not.
Static traction — like hanging upside down or using a mechanical traction device — applies a constant pull to the spine. The problem is that your body's natural response to being stretched is muscle guarding. Your muscles contract to protect the spine from what they perceive as a threat.
That muscle contraction increases pressure inside the disc — the exact opposite of what you're trying to achieve.
Non-invasive disc recovery uses computer-controlled cycles of tension and release. The machine pulls, then releases slightly, then pulls again — in a rhythm designed to bypass the muscle guarding response. The result is sustained negative pressure without triggering the body's protective reflex.
That's the difference between a $200 inversion table and a clinical decompression protocol. One creates static tension. The other creates a controlled pressure gradient that actually changes intradiscal mechanics.
| Method | Pressure Control | Muscle Guarding Response | Intradiscal Pressure Change |
|---|---|---|---|
| Inversion Table | None — static gravitational pull determined by body weight and angle | High — sustained stretch triggers protective muscle contraction | Minimal or counterproductive — muscle guarding can increase intradiscal pressure |
| Manual Traction (PT) | Limited — therapist applies steady pull, cannot modulate pressure in real-time | Moderate — therapist can adjust based on patient feedback, but muscle guarding often occurs | Slight reduction possible, but difficult to sustain negative pressure threshold |
| Computer-Controlled Decompression | Precise — tension cycles programmed to bypass guarding reflex, pressure monitored continuously | Low — rhythmic pull-and-release pattern prevents sustained muscle contraction | Significant negative pressure achieved — creates vacuum effect to retract disc material |
When Physical Therapy Is The Right Choice
Here's the thing: this isn't an anti-PT article.
PT is a legitimate, evidence-based treatment for the right conditions.
The problem is when it's applied to the wrong problem.
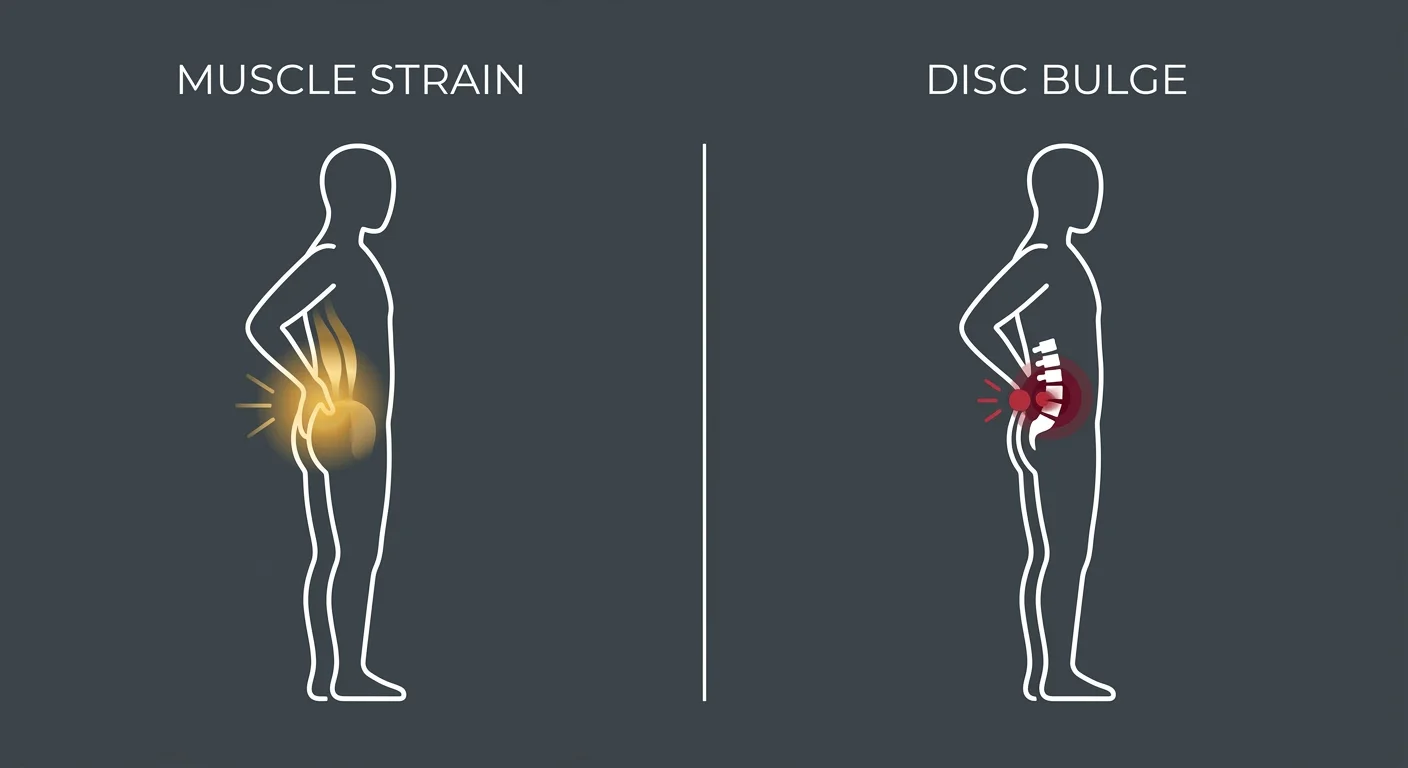
Muscle Strains and Postural Issues
If your back pain is coming from a muscle strain — an overstretched lumbar muscle, a trigger point in the erector spinae, or chronic tension from poor posture — PT is often the correct first-line treatment.
Muscle injuries respond to stretching, strengthening, and activity modification. A good physical therapist can identify movement patterns that are causing the strain and teach you how to move differently. They can prescribe exercises that restore muscle balance and prevent future injury.
PT is also highly effective for postural dysfunction. If your pain is caused by sitting at a desk for 10 hours a day with your shoulders rounded and your pelvis tilted forward, you don't need spinal decompression. You need someone to teach you how to sit, stand, and move with better alignment.
The key distinction: if your pain is muscular or postural in origin, PT targets the root cause. If your pain is coming from a compromised disc, PT targets the symptoms.
Post-Surgical Rehabilitation
Physical therapy is absolutely essential after disc surgery — whether that's a microdiscectomy, laminectomy, or spinal fusion.
Once the structural problem has been corrected surgically, PT helps you rebuild the strength and mobility you lost during recovery. It teaches you how to move safely with your new spinal anatomy. It prevents compensatory movement patterns that could cause problems elsewhere in the kinetic chain.
In this context, PT isn't trying to fix the disc. The disc has already been fixed — or removed. PT is rebuilding the system around it.
That's a completely different clinical goal — and it's one PT is designed to achieve.
The Complementary Role
Sometimes PT and non-invasive disc recovery work together.
You need decompression to address the disc itself, and you need PT to maintain the stability that prevents re-injury.
The difference is timing and priority. If the disc is the problem, decompression comes first. Once the disc is healing and nerve symptoms are resolving, PT can support that progress by strengthening the stabilizers and improving movement quality.
But if you're doing PT first and the pain keeps coming back, you're treating the wrong layer. You're strengthening the container while the contents are still broken.
The Assessment That Determines Your Path
You don't know if you need disc recovery or PT until someone actually looks at your case.
Not a quick exam. Not a 10-minute intake. A real assessment.
What the Initial Evaluation Reveals
The evaluation starts with history.
How did the pain start? Is it constant or intermittent? Does it radiate? What makes it better or worse? How long have you been dealing with it? What've you already tried?
Those answers tell you more than most imaging ever will.
Then comes orthopedic testing. Straight leg raise to check for nerve tension. Reflex testing to see if nerve conduction is impaired. Range of motion assessment to identify where the restriction is coming from. Palpation to rule out muscular referral patterns.
If you've had imaging — an MRI or CT scan — that gets reviewed. But here's the thing: imaging alone doesn't determine treatment. Plenty of people have bulging discs on MRI and zero symptoms. And plenty of people have severe pain with minimal findings on imaging.
The assessment is looking for clinical correlation. Does your pain pattern match what the imaging shows? Do your neurological findings suggest nerve involvement? Is the disc the primary driver, or is this a muscular compensation issue?
That's what determines candidacy for non-invasive disc recovery. Not a diagnosis code. Not a referral. A clinical picture that says: the disc is the problem, and decompression is the right tool.
If you've had a chiropractic adjustment before and it helped temporarily but didn't resolve the problem, that's often a sign that the disc itself needs direct intervention — not just spinal mobilization.
When Disc Recovery Is Not the Answer
Not everyone is a candidate for spinal decompression.
And that matters.
If your pain is primarily muscular, you don't need decompression. If you have severe spinal instability or fractures, decompression isn't safe. If you've had a recent spinal fusion, you're not a candidate. If you have advanced osteoporosis, the traction forces could cause more harm than good.
And here's the other disqualifier: if you're not willing to commit to the full care plan, this isn't for you.
Disc recovery is not a one-and-done session. It's not something you try for a week and bail on if you don't feel better immediately. It's a structured care plan that requires consistent sessions over a period of weeks — sometimes months — depending on the severity of the injury.
If you're the type of person who picks and chooses which parts of the plan to follow, you're setting yourself up for partial results. And partial commitment to disc recovery is worse than not starting at all — because you'll walk away thinking it didn't work, when the reality is you didn't give it a chance to work.
That's The Plan Picker problem. Selective compliance produces selective results. If you're not willing to show up clinically and financially for the duration of the care plan, that's important information for both of us to have up front.
The Care Plan That Fits What You Actually Need
If the assessment determines that disc recovery is the right path, the care plan is built from your clinical picture.
Not from a billing calendar. Not from what the last patient needed. From what your case actually requires.
Some patients need 15 sessions. Some need 25. Some need ongoing maintenance after the acute phase resolves. The plan changes if something isn't producing results.
That's not a failure of the protocol — that's clinical responsiveness.
"But doesn't my doctor say PT is the gold standard?"
Your doctor is right — for muscle strains, postural dysfunction, and post-surgical rehab. But if you've already done PT and the pain came back, the gold standard for your case wasn't PT. It was the wrong tool for the actual problem.
"Isn't non-invasive disc recovery just unproven traction that doesn't work?"
Static traction doesn't work because it triggers muscle guarding. Computer-controlled decompression works because it bypasses that reflex and creates sustained negative pressure. The research exists. The mechanism is sound. The question is whether your case fits the profile.
If you're dealing with nerve-related conditions that haven't responded to standard care, this is worth a conversation. Not because it's always the answer. But because when it is, everything else starts making sense.
FAQ
Can physical therapy make a herniated disc worse?
It's rare, but it can happen — especially if the exercises are performed incorrectly or if the protocol increases pressure on the disc.
A skilled physical therapist will modify exercises based on your response. But generic PT programs that apply the same sequence to every patient don't account for individual variability. If an exercise causes sharp radiating pain, numbness, or increased leg symptoms, that's a sign the disc is being aggravated.
That's why individualized assessment is critical. The goal of PT is to improve function without worsening the underlying injury. If pain increases during or after PT sessions, the protocol needs to be reassessed — not repeated.
How is non-invasive disc recovery different from simple inversion tables or traction?
Inversion tables and manual traction apply a constant static pull. Your body's natural response to that pull is muscle guarding — the muscles contract to protect the spine, which increases intradiscal pressure. That works against the goal.
Non-invasive disc recovery uses computer-controlled tension that cycles between pull and release. This rhythmic pattern bypasses the muscle guarding reflex, allowing sustained negative pressure to develop inside the disc. That negative pressure is what retracts herniated material and draws in healing nutrients.
Static traction creates tension. Decompression creates a pressure gradient. That's not a marketing difference. It's a mechanical difference.
Do I need a doctor's referral for non-invasive disc recovery?
No. In Illinois, you do not need a referral from a medical doctor to have a chiropractic assessment for spinal decompression therapy.
The chiropractor will conduct a full evaluation — including history, orthopedic testing, and imaging review if available — to determine if you're a candidate for care. If you're not a good fit, that will be stated clearly during the consultation.
The assessment is what determines the path forward. Not a referral. Not a diagnosis code handed over from another provider. Your actual clinical presentation.
If my core is already strong, why would I still have disc pain?
Because a strong core supports the structure. It doesn't fix what's happening inside the disc.
Core strength is crucial for spinal stability. It reduces the load on your discs during movement. It prevents compensatory patterns that could cause injury elsewhere. All of that matters.
But if the disc is already herniated — if the nucleus pulposus has already broken through the annular fibers and is compressing a nerve — no amount of core strength will retract that material. Muscle strength is external to the disc. The herniation is internal.
You need both. Core strength prevents re-injury once the disc heals. But decompression is what creates the conditions for the disc to heal in the first place.
How long does it take to see results with non-invasive disc recovery?
Most patients begin to experience relief within the first few weeks of care. Nerve symptoms — radiating pain, numbness, tingling — often improve first, because the disc material starts retracting away from the nerve root.
But early relief is not full resolution. The disc itself takes longer to heal. That's why the full care plan is designed to promote long-term healing, not just temporary symptom reduction.
The timeline varies based on the severity of the injury, how long you've been dealing with it, and how well you respond to treatment. Some patients feel significantly better after 10 sessions. Others need 20 or more before the disc stabilizes.
The goal is not speed. The goal is complete resolution. And that requires committing to the process.
What happens if I stop physical therapy and try disc recovery instead?
If you've been doing PT for weeks or months and the pain keeps coming back, stopping PT to try disc recovery isn't abandoning a successful treatment. It's pivoting from a tool that didn't work to a tool that might.
The assessment will determine if disc recovery is the right next step. Sometimes PT was the wrong approach from the start. Sometimes PT helped stabilize the area but couldn't address the disc itself. Sometimes both approaches have complementary roles — decompression first, then PT to maintain the results.
The key is being honest about what's actually happening. If PT worked, you wouldn't be reading this. If it didn't work, doing more of it won't change the outcome.
Conclusion
If physical therapy worked, your disc pain would be gone by now.
It's not.
You've done the exercises. You've stretched. You've modified your activity. You've been patient. And the pain came back anyway — because PT was treating the muscles around the disc, not the disc itself.
That's not a failure of effort. It's a failure of tool selection. You can't muscle your way out of a mechanical pressure problem. You can't strengthen your way around a herniated disc that's still compressing a nerve.
When a treatment isn't working and you keep doing it anyway, that's not persistence. That's the clinical definition of failure.
Non-invasive disc recovery targets the one thing PT cannot touch: intradiscal pressure. It creates the mechanical conditions the disc needs to retract, decompress, and heal. It doesn't manage the symptoms. It resolves the cause.
If you've been dismissed, told to keep doing your exercises, or handed a timeline that never explained the why — this is a different conversation. The disc is the problem. Decompression is the tool. And the assessment will tell you if it's the right fit for your case.
If you've done PT and the disc pain keeps coming back, that's worth a real conversation.
A chiropractic assessment at Touch of Wellness Chiropractic starts with what you actually report — not a standard protocol handed over before the evaluation is even finished. The goal is to determine if the disc is the problem, if decompression is the right tool, and what your care plan actually needs to look like.
If you're in Morton, Peoria, or the surrounding area and you're done managing symptoms that won't stay fixed, find out what your assessment looks like.
PT strengthens the container. Disc recovery changes what's inside it. When the disc is the problem, that distinction is everything.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet