
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
(309) 321-8412 | 1101 W Jackson St, Suite A, Morton, IL 61550
Why Core Strength Alone Can't Fix a Lumbar Disc Injury
Core strength alone cannot fix a lumbar disc injury because it fails to address the underlying mechanical fault in the spine that created the injury in the first place. A herniated or bulging disc is a structural problem where the inner part of the disc material pushes through the outer layer, often putting pressure on nearby nerves. This isn't caused by weak abdominal muscles—it's caused by spinal joint dysfunction, inflammation, and abnormal loading patterns at the affected segment.
You've been doing the core work. Every day. And your back still feels unstable when you bend over. That's not because you're not trying hard enough. It's because a strong core provides external support, but it cannot correct the specific mechanical problem at the joint level. And more critically, it cannot restore the nervous system's ability to properly signal the deep stabilizing muscles that control individual vertebrae. These muscles—the lumbar multifidus, psoas major, and others—are responsible for segmental spinal stability, which is completely different from the global "core strength" developed through planks and crunches. When spinal joint motion is restricted or misaligned, the brain's ability to coordinate these stabilizers becomes impaired, even if the superficial abdominal muscles are strong.
True recovery from a lumbar disc injury requires a different sequence. First, spinal joint function must be restored through targeted chiropractic adjustments that reduce nerve interference and improve segmental motion. This allows the nervous system to properly activate the deep stabilizers again. Second, inflammation around the disc must be addressed to reduce pressure and pain. Third—and only after these foundational issues are corrected—can strengthening exercises be effective. Trying to build core strength on top of a dysfunctional spinal joint is like trying to add a new wall to a cracked foundation. The structure will fail no matter how strong the materials are, because the base is compromised.
The problem isn't that core exercises are bad. The problem is that they're being prescribed at the wrong stage of recovery, to address a problem they were never designed to solve. A disc injury is a mechanical issue that requires a mechanical solution. Core strengthening is a Stage 2 or Stage 3 intervention. If it's the only tool being used—or if it's being used first—it will fail. And in many cases, it can make the injury worse by increasing intra-discal pressure before the spine is ready to handle that load.
Last Updated: April 30, 2026
- The Core Strength Trap: Why the Standard Protocol Fails
- What Actually Happens in a Lumbar Disc Injury
- The Missing Link: Nervous System Control of Spinal Stability
- Why Core Exercises Can Make a Disc Injury Worse
- What Real Disc Recovery Looks Like
- Frequently Asked Questions
- The Foundation Must Be Fixed First
The Core Strength Trap: Why the Standard Protocol Fails

You've been doing the exercises. Every morning.
The planks, the bridges, the bird dogs. Your physical therapist said core strength was the answer. Your doctor said the same thing. "Strengthen your core and the pain will go away."
But it didn't.
The pain's still there. Sometimes it backs off for a few days, then comes roaring back worse than before. You're doing everything right, but nothing's actually fixing it.
That's not because you're doing the exercises wrong. It's because the exercises are the wrong tool for what's actually broken.
Why "Strengthen Your Core" Is Cookie-Cutter Advice
Most PT offices run the same routine on every disc injury that walks through the door.
Walk in with a herniated disc. Walk in with sciatica. Walk in with chronic instability. Doesn't matter — you get the same sheet of exercises. Planks. Bridges. Dead bugs. Six weeks of the same protocol.
That's a template. It's designed for efficiency, not precision.
And it completely ignores the mechanical reality of your injury. Your disc didn't herniate because your abs were weak. It herniated because something in your spine wasn't moving correctly — repetitive loading on a faulty joint, a restriction that never got addressed, or trauma that created an uneven stress pattern.
The disc failed because the structure around it was already compromised.
Telling you to strengthen your core is like telling you to reinforce the walls of a house while the foundation's cracked. The walls might look better, but the structure's still failing from the bottom up.
The Real Problem: Joint Dysfunction, Not Muscle Weakness
Here's what actually happens before a disc herniates.
The vertebrae above or below the disc stop moving correctly. Maybe it's from poor posture. Maybe it's from repetitive bending. Maybe it's an old injury that never fully healed. The joint becomes restricted or misaligned.
When one joint doesn't move, the joints around it compensate. They move too much.
The disc between those vertebrae takes the load unevenly. Over time, that repetitive stress weakens the outer layer. Eventually, it tears. The inner gel-like material pushes through. That's the herniation.
The disc didn't fail because your muscles were weak. It failed because the mechanical structure was faulty.
And until that mechanical fault is corrected, no amount of core strengthening will fix it.
At Touch of Wellness Chiropractic, individualized, root-cause chiropractic care starts with identifying the exact joint causing the problem. Not a generalized "your back is weak" diagnosis. A specific assessment of which vertebra isn't moving correctly and why.
| Factor | Core Strength (Global) | Spinal Stability (Segmental) |
|---|---|---|
| Muscles Involved | Rectus abdominis, obliques, hip flexors—large trunk muscles you can consciously contract | Multifidus, transverse abdominis, psoas major—small muscles close to the spine that stabilize individual vertebrae |
| Controlled By | Voluntary movement—you decide to engage them during an exercise | Nervous system reflexes—activated automatically in response to spinal joint motion and sensory feedback |
| Function | Generate force to move or hold the trunk in position—rotation, flexion, resisting external loads | Protect and stabilize each individual spinal segment during movement—prevents excessive motion at any one joint |
| Developed Through | Exercises like planks, crunches, leg raises—anything that loads the trunk muscles under conscious effort | Proper spinal joint mechanics first, then targeted movement retraining once nerve signaling is restored |
| Role in Disc Injury Recovery | Stage 3—after joint function and nerve control are corrected, global strengthening helps prevent re-injury | Stage 1—the foundation that must be restored before any strengthening work can be effective |
What Actually Happens in a Lumbar Disc Injury

The disc sits between two vertebrae. It's made of two parts — a tough outer ring called the annulus fibrosus, and a gel-like center called the nucleus pulposus.
When the spine moves correctly, the disc compresses and expands evenly. The pressure distributes across the entire surface.
But when one vertebra doesn't move right, the pressure becomes uneven. It concentrates on one side of the disc.
Over time, the outer ring starts to weaken. Cracks form. The inner gel pushes through those cracks. That's a herniation.
This is a mechanical event. Not a muscular one.
The Mechanical Fault: Abnormal Joint Motion
Disc injuries don't happen in isolation.
They happen because the vertebrae above or below the disc aren't moving correctly. Maybe the facet joints are restricted. Maybe the vertebra's slightly rotated or tilted. Whatever the cause, the result's the same — repetitive stress on a joint that can't handle it.
Over time, the disc fails.
Stretching doesn't fix this. Strengthening doesn't fix this. Both can help once the joint's moving correctly again, but if the mechanical fault's still there, the disc will keep breaking down.
According to Cleveland Clinic, a herniated disc occurs when the inner portion protrudes through a tear in the outer layer, often pressing on nearby nerves and causing pain, numbness, or weakness.
The National Institute of Neurological Disorders and Stroke confirms that low back pain is often caused by mechanical issues in the spine, and recovery focuses on restoring proper function to prevent re-injury.
Nerve Compression and Inflammation
When the disc bulges, it often puts pressure on a nerve root.
That pressure creates the classic symptoms — shooting pain down the leg, numbness in the foot, tingling in the toes. Sciatica.
But here's what most people don't realize. That nerve isn't just carrying pain signals. It's also carrying motor signals — the commands from your brain to your muscles.
When a nerve's compressed, those motor signals get disrupted.
The brain tries to activate the deep stabilizing muscles around the spine, but the signal doesn't get through clearly. The result? Even if you're doing the exercises correctly, the muscles don't fire the way they're supposed to.
You can feel your abs working. You can hold a plank. But your back still feels unstable.
That's because the instability isn't coming from weak muscles. It's coming from poor nerve signaling caused by the compressed nerve root.
Chiropractic care that restores nervous system function addresses this directly — removing the mechanical interference so the nerve can function correctly again.
The Missing Link: Nervous System Control of Spinal Stability
The spine isn't just a stack of bones. It's a neurological structure.
Every movement, every stabilization response, every micro-adjustment your body makes to keep you upright — all of it's controlled by the nervous system.
When spinal joints move correctly, the mechanoreceptors in those joints send feedback to the brain. The brain uses that feedback to coordinate the muscles that stabilize the spine.
It's a constant loop. Movement creates feedback. Feedback drives muscle coordination. Muscles control movement.
But when a spinal joint's restricted or misaligned, that feedback loop breaks down.
The brain doesn't get accurate information from the mechanoreceptors. Without accurate information, it can't coordinate the stabilizing muscles correctly. The deep stabilizers — the multifidus, the psoas major, the transverse abdominis — stop firing the way they're supposed to.
This is where my Zoology background matters. The spine is a biological system. It's not isolated. It's integrated.
If one part of the system isn't functioning, the entire system compensates. And no amount of external strengthening will fix an internal control problem.
If you're someone who expects the provider to fix everything while you do nothing between appointments, we're probably not the right fit. Recovery requires both parties showing up.
But if you've been doing the exercises your last provider gave you and they're not working — that's not your fault. That's a sign the exercises were prescribed at the wrong stage, for a problem they were never designed to solve.
Deep Stabilizers vs. Global Movers
There are two types of muscles that control the spine.
Global movers are the big ones. Rectus abdominis. Obliques. Hip flexors. You can feel them working when you do a crunch or hold a plank. They generate force. They move the trunk.
Deep stabilizers are small. Multifidus. Psoas major. Transverse abdominis.
They sit close to the spine and control individual vertebrae. You can't consciously "activate" them the way you can flex your abs.
They're controlled almost entirely by reflex arcs through the nervous system. They respond to proper joint motion and accurate nerve signaling.
Research published by the National Institutes of Health shows that the lumbar multifidus and psoas major muscles are critical for segmental spinal stability — a function that's completely distinct from general "core strength."
When spinal joints aren't moving correctly, the brain can't coordinate the deep stabilizers.
Even if the global movers are strong, the spine remains unstable at the segmental level. That's why you can have a six-pack and still have chronic low back pain. The problem isn't strength. It's control.
Why Your Body Won't Stabilize a Broken Joint
The nervous system is protective.
If a joint isn't moving correctly, the brain won't allow full muscle activation around it. It's a safety mechanism. Forcing full activation on a compromised joint could cause more damage, so the body limits the response.
This is why so many patients say, "I can feel my core muscles working, but my back still feels unstable."
The instability's coming from the joint, not the muscle.
Until the joint's corrected, the muscle won't fully engage. And no amount of exercise will override that protective response.
| Stage | What's Happening | Why Core Work Doesn't Help |
|---|---|---|
| Stage 1: Acute Injury | Disc has herniated, nerve is compressed, inflammation is high, spinal joint is restricted or misaligned | Core exercises increase intra-discal pressure and can worsen the herniation; nervous system won't activate stabilizers around a compromised joint |
| Stage 2: Inflammation | Pain is present but not constant, movement is limited by guarding and muscle spasm, nerve compression may still be active | Strengthening exercises are painful and counterproductive; the body is trying to protect the area, and loading it prematurely delays healing |
| Stage 3: Chronic Dysfunction | Pain has been present for months or years, joint motion is still restricted, deep stabilizers have atrophied from disuse, compensatory patterns are established | Without restoring joint mechanics first, core exercises only reinforce compensatory patterns; the weak link in the chain is still broken |
Why Core Exercises Can Make a Disc Injury Worse
Your doctor told you to strengthen your core. Your physical therapist gave you a list of exercises.
But every time you do them, it hurts more.
You're not doing them wrong. The exercises are wrong for this stage of recovery.
The Cookie-Cutter Protocol Problem
Walk into most PT offices with a disc injury, and you'll get the same sheet. Crunches. Sit-ups. Planks. Leg raises.
These exercises work — after the joint's been corrected. Before that, they're the wrong tool at the wrong stage. Doing them early doesn't accelerate recovery. It delays it.
But for someone with a herniated disc and compromised joint mechanics, they're the exact wrong prescription.
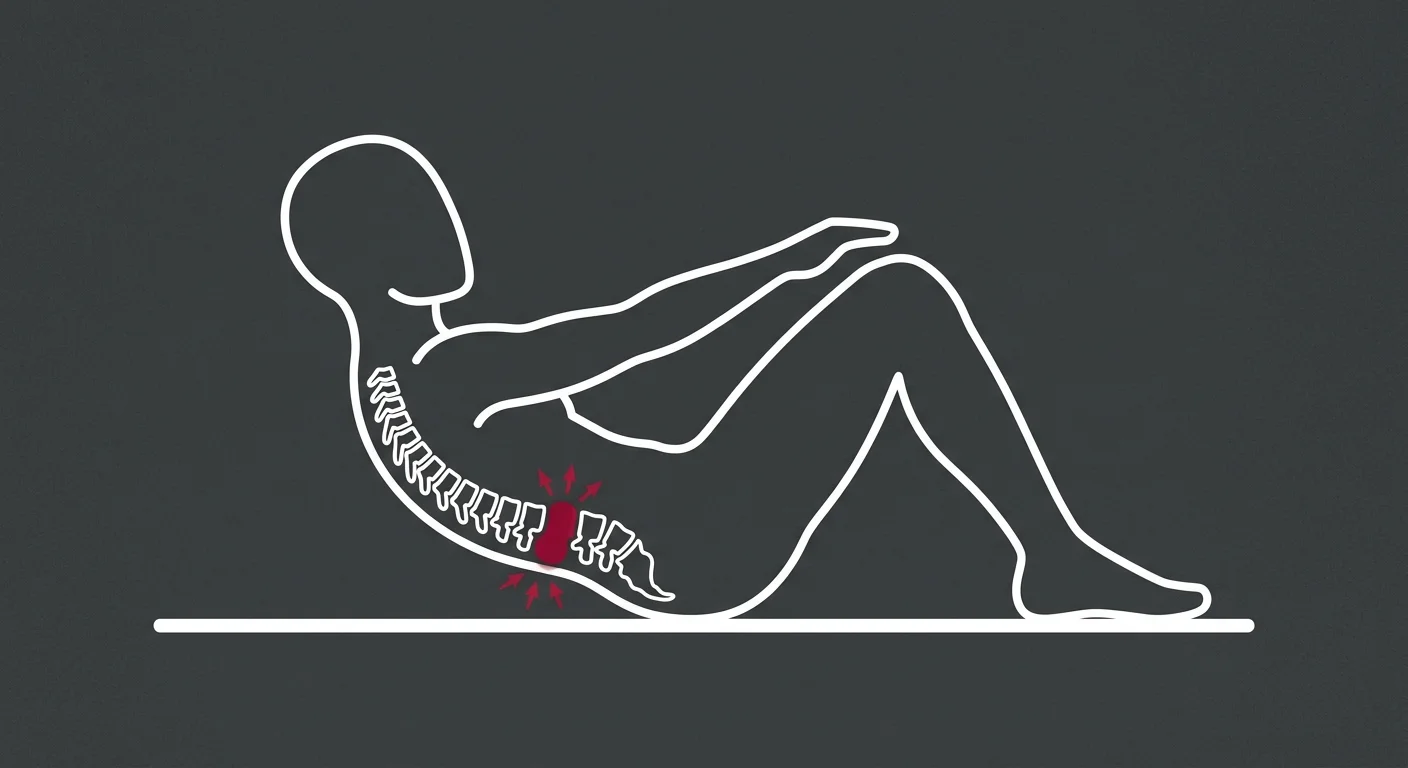
Why? Because they all involve spinal flexion under load. And spinal flexion dramatically increases the pressure inside the disc.
Research published in the International Journal of Sports Physical Therapy shows that effective core stabilization involves more than just the abdominal muscles — it includes the diaphragm, pelvic floor, and deep spinal muscles. But standard PT protocols often skip past the foundational work and jump straight to the global exercises.
That's the cookie-cutter protocol. Same exercises for every patient. No adjustment for the mechanical reality of the injury.
If the patient reports that the exercises aren't working — or that they're making things worse — the response is usually, "Keep doing them. It takes time."
That's not care. That's guesswork.
If something isn't producing results after a few visits, it changes. Not repeated. Changed. The willingness to stop and reassess isn't a weakness. It's the whole point.
Exercises That Increase Disc Pressure
Any exercise that involves spinal flexion under load increases the pressure inside the disc.
Crunches. Sit-ups. Certain types of planks. Leg raises. Forward bends.
When you flex the spine, the front of the disc compresses and the back of the disc expands. If the disc's already compromised — if there's a tear in the outer layer — that increased pressure can push more nucleus material out through the tear.
The herniation gets worse. The nerve compression increases. The pain intensifies.
This isn't theoretical. It's measurable.
Intra-discal pressure studies have shown that flexion-based exercises create the highest loads on the lumbar discs. If your disc's already injured, these exercises are making it harder to heal.
The Psoas Problem
The psoas major muscle runs from the lumbar spine to the femur. It's one of the primary hip flexors, and it's also one of the deep stabilizers of the lumbar spine.
When the psoas is tight or imbalanced, it pulls the lumbar vertebrae forward. That increases the anterior pressure on the discs.
Over time, that pressure contributes to disc degeneration and herniation.
Many "core strengthening" programs include hip flexor exercises — leg raises, mountain climbers, running in place. These exercises can tighten the psoas further.
If spinal alignment hasn't been corrected first, strengthening the psoas just makes the problem worse.
According to Spine-health, an imbalanced or tight psoas muscle can pull the lumbar spine out of alignment, contributing to disc pressure regardless of abdominal strength.
| Exercise Type | Avoid (Why) | Safe Alternative | When to Progress |
|---|---|---|---|
| Flexion Exercises (crunches, sit-ups, toe touches) | Dramatically increase intra-discal pressure; can worsen herniation by pushing nucleus material posteriorly | Neutral spine holds (quadruped position, modified plank on knees) | Only after spinal mechanics are corrected and nerve compression is resolved—typically 4-6 weeks into care |
| Rotation Under Load (Russian twists, standing wood chops with weight) | Creates shear forces on the disc; can aggravate tears in the annulus fibrosus | Controlled rotation in neutral spine without load (standing torso rotation, arm swings) | After pain-free range of motion is restored and deep stabilizers are firing correctly |
| Heavy Lifting (deadlifts, squats with significant weight) | Compressive forces exceed the disc's capacity to heal; risk of re-injury or worsening herniation | Bodyweight squats, wall sits, isometric holds | Only after full function is restored and patient has completed at least 8-12 weeks of progressive stability training |
| Static Holds in Flexion (long-duration forward bends, child's pose held for extended periods) | Sustained flexion prevents proper nutrient exchange in the disc; delays healing | Short-duration stretches in neutral or slight extension (cobra pose, standing extension) | After acute inflammation resolves and patient can tolerate movement without increased pain |
What Real Disc Recovery Looks Like
Real disc recovery happens in stages. Not random stages. Not interchangeable stages.
A specific sequence.
Stage 1: Restore spinal joint function through chiropractic adjustment. This reduces nerve compression, decreases inflammation, and allows the nervous system to begin signaling the stabilizers again.
Stage 2: Address inflammation and pain through advanced modalities. Cold Laser Therapy. Acupuncture. Shockwave Therapy. These aren't optional add-ons — they're tools that accelerate tissue healing and reduce chronic nerve irritation.
Stage 3: Once mechanics and nerve function are restored, introduce targeted stability exercises. Not the same exercises you were doing before. Specific movement patterns designed to retrain the deep stabilizers under proper joint mechanics.
The sequence matters.
Skip Stage 1 and Stage 2, and Stage 3 will fail every time. That's what the fifteen-minute disc restoration protocol at Touch of Wellness Chiropractic is built around — addressing the root cause first, not masking symptoms.
Stage 1: Spinal Joint Correction
A chiropractic adjustment restores proper motion to a restricted or misaligned joint.
This isn't about "cracking your back." It's about removing the mechanical interference that's preventing the disc from healing and the nervous system from functioning correctly.
When the joint moves correctly, three things happen.
One: Pressure on the disc distributes evenly again. The herniation stops progressing.
Two: Nerve compression decreases. The nerve can start sending clear motor signals to the muscles again.
Three: The mechanoreceptors in the joint start sending accurate feedback to the brain. The brain can begin coordinating the deep stabilizers.
That's the foundation. Without it, nothing else works.
If you're wondering when to see a chiropractor for lower back pain, the answer is this: when the pain's been present long enough that it's disrupting your daily life, and when standard medical care hasn't addressed the mechanical cause.
Stage 2: Reducing Inflammation and Nerve Pressure
Inflammation is both a symptom and a perpetuating factor.
When a disc herniates, the body's immune system responds. Inflammatory chemicals flood the area. They're supposed to help healing, but in chronic cases, they just keep the nerve irritated.
That's where advanced modalities come in.
Shockwave Therapy uses acoustic waves to stimulate tissue healing and reduce chronic inflammation. It accelerates the body's natural repair process — without drugs, without injections.
Cold Laser Therapy reduces pain and inflammation at the cellular level. Acupuncture improves blood flow and reduces muscle tension around the affected area.
These aren't just pain management tools. They're recovery tools.
They create the conditions for the disc to heal and the nerve to decompress. The conditions Shockwave Therapy can treat include chronic low back pain, sciatica, and nerve-related conditions that haven't responded to standard care.
Stage 3: Stability Training (Once the Foundation Is Fixed)
After spinal mechanics are corrected and nerve function is restored, targeted exercises become effective.
But these aren't the same exercises you were doing before.
They're not crunches. They're not planks. They're not high-rep, high-intensity circuits.
They're specific movement patterns designed to retrain the deep stabilizers under proper joint mechanics. The nervous system can now coordinate them correctly because the interference has been removed.
This is where physical therapy becomes effective — when it's applied at the right stage, after the mechanical fault has been corrected.
But if you jump straight to this stage without fixing the foundation first, you're just reinforcing compensatory patterns. The weak link in the chain is still broken.
But Doesn't My Core Still Need to Be Strong?
Yes. Absolutely.
But strength without stability is useless. And stability without proper mechanics is impossible.
The sequence matters.
If you build strength on top of a dysfunctional joint, that strength becomes part of the problem. The muscles learn to compensate. They adapt to the faulty mechanics.
Over time, those compensations become so ingrained that even when the joint's corrected, the muscles don't know how to fire correctly anymore.
That's why trying to "strengthen your way out" of a disc injury fails. You're teaching your body to be really good at moving incorrectly.
Fix the mechanics first. Then build strength on top of a stable foundation.
Why the 15-Minute Standard Matters
The 15-minute door-to-door standard at Touch of Wellness Chiropractic isn't about rushing through appointments.
It's about precision.
The assessment identifies the exact spinal segment causing the problem. The adjustment is targeted. The care plan is built from what the patient actually reports — not from a template.
If something isn't producing results after a few visits, the approach changes. Not repeated. Changed.
That willingness to reassess — not just run the same protocol and hope it eventually works — is what separates root-cause care from cookie-cutter care.
The difference between Non-Invasive Disc Recovery and traditional physical therapy isn't that one's better than the other. It's that they address different problems at different stages. Physical therapy is excellent for muscle re-education. But if the joint mechanics and nerve function haven't been addressed first, the exercises can't be fully effective.
Frequently Asked Questions
Can crunches or planks make my disc herniation worse?
Yes. Both exercises involve spinal flexion under load, which increases intra-discal pressure.
When you do a crunch, you flex the lumbar spine forward. That compresses the front of the disc and expands the back. If the disc's already compromised — if there's a tear in the outer layer — that increased pressure can push more nucleus material out through the tear.
The herniation gets worse. The pain intensifies. The nerve compression increases.
Research published in the International Journal of Sports Physical Therapy confirms that flexion-based exercises significantly increase disc pressure and should be avoided during the acute and subacute phases of a disc injury.
Planks are safer than crunches, but only if you maintain a perfectly neutral spine. Most people can't. As fatigue sets in, the pelvis tilts and the lumbar spine flexes. That's when the pressure spikes.
These exercises aren't bad. They're just the wrong tool during the acute recovery phase.
After spinal mechanics are corrected and the disc has stabilized, they can be reintroduced gradually. But not before.
Is it possible for my core to be strong, but my back still be unstable?
Absolutely. This is one of the most common patterns I see.
You can do a two-minute plank. You can hold a perfect hollow body position. But your back still feels unstable when you bend over to pick something up, or when you get out of bed in the morning.
That's because core strength and spinal stability are not the same thing.
Core strength refers to the force-producing capacity of your trunk muscles. Rectus abdominis. Obliques. Hip flexors. These are the muscles you can consciously contract during an exercise.
Spinal stability is the nervous system's ability to coordinate all the muscles around the spine — including the deep stabilizers — to protect each individual joint through its range of motion.
You can have strong "mover" muscles and weak, uncoordinated "stabilizer" muscles.
That happens when spinal joint dysfunction disrupts the nerve signaling to the deep stabilizers. The brain can't activate them correctly, even if you're doing the exercises.
The instability you're feeling isn't coming from weak abs. It's coming from poor segmental control at the joint level.
What's the difference between core strength and spinal stability?
Core strength is about force production. How much load can your trunk muscles handle? How long can you hold a position against resistance?
Spinal stability is about control.
Can your nervous system coordinate the muscles around each individual vertebra to prevent excessive motion at any one joint?
Core strength is conscious. You decide to engage your abs during a plank. You feel the burn. You can measure progress by how long you can hold the position.
Spinal stability is reflexive. It happens automatically in response to movement and load.
The deep stabilizers fire before the global movers, creating a protective brace around the spine before you even start moving.
You can train core strength with standard exercises. Crunches, planks, leg raises. But you can't train spinal stability with those exercises if the spinal joints aren't moving correctly and the nervous system isn't coordinating the stabilizers properly.
Research from the National Institutes of Health shows that the lumbar multifidus and psoas major muscles are critical for segmental spinal stability — a function that's completely distinct from general "core strength."
That's why someone can have a six-pack and still have chronic low back pain. The problem isn't strength. It's control.
How does a chiropractic adjustment help a disc injury if it's not a muscle problem?
Because a disc injury is a mechanical problem, and a chiropractic adjustment is a mechanical solution.
The adjustment restores proper motion to the restricted or misaligned spinal joint. That does three things.
One: It reduces the abnormal stress on the disc. When the joint moves correctly, the disc is no longer being loaded unevenly. That allows it to begin healing.
Two: It reduces pressure on the nerve root. When the vertebra shifts back into alignment, the nerve has more space. The compression decreases. The pain, numbness, and tingling start to resolve.
Three: It restores proper feedback from the mechanoreceptors in the joint. The brain starts receiving accurate information again. That allows it to coordinate the deep stabilizing muscles correctly.
According to Mayo Clinic, medical treatment for disc problems often involves addressing inflammation and nerve pressure — not just muscle weakness.
The adjustment addresses the root cause of the injury: the mechanical fault that created the uneven loading in the first place.
That's why patients often report immediate improvement in symptoms after an adjustment. The mechanical interference has been removed. The nervous system can function correctly again.
If I've already done physical therapy, can chiropractic care still help?
Yes. Many patients come to chiropractic care after completing a full course of physical therapy with minimal or no improvement.
Physical therapy is excellent for muscle re-education and strengthening. But if the underlying joint mechanics and nerve function weren't addressed first, the exercises can't be fully effective.
This isn't a failure of physical therapy. It's a sequence issue.
If you give someone the right exercises at the wrong stage of recovery, they won't work. The body isn't ready for them yet. The foundation isn't stable.
Chiropractic care addresses the foundation — the spinal joint function and nervous system control that must be restored before strengthening exercises can be effective.
Many patients find that after a few weeks of chiropractic care, the same exercises that didn't work during PT suddenly start producing results.
That's because the mechanical interference has been removed. The nervous system can coordinate the muscles correctly now.
This is why the comparison between Non-Invasive Disc Recovery and traditional physical therapy isn't about which approach is better. It's about which approach addresses the specific problem at the specific stage of recovery you're in right now.
How long does it take to recover from a lumbar disc injury?
It depends on three factors: how severe the injury is, how long it's been present, and how quickly joint function and nerve signaling can be restored.
Some patients see significant improvement in 2-4 weeks. These are usually cases where the injury's recent, the disc hasn't fully herniated, and the nerve compression is minimal.
Others with chronic, long-standing injuries may take 8-12 weeks.
These cases often involve multiple compensatory patterns, muscle atrophy, and significant nerve irritation that's been present for months or years.
The key is addressing the root cause — not masking symptoms.
A care plan built around symptom management can drag on for months with minimal progress. A care plan built around restoring spinal mechanics and nerve function produces measurable improvement within the first few weeks.
If a patient isn't seeing improvement after 3-4 visits, the approach changes. That's the standard. Not six months of the same protocol with vague promises that "it takes time."
If you're being told to keep doing the same exercises for months with no clear improvement timeline, that's not a care plan. That's hope disguised as strategy.
The Foundation Must Be Fixed First
The nervous system runs everything.
When a spinal joint's dysfunctional, the entire system compensates. The deep stabilizers stop firing correctly. The global movers take over. Compensatory patterns become ingrained.
Over time, those patterns create new problems in other areas of the spine.
Core strength is valuable. But only after the foundation is stable.
Trying to build strength on top of a mechanical fault isn't a patient failure. It's a clinical failure.
If you've been told to "just keep doing your exercises" and the pain hasn't resolved, that's not a sign you need to work harder. It's a sign the approach is wrong.
Unexplained doesn't mean untreatable. It means no one's looked at the right thing yet.
The disc didn't herniate because your abs were weak. It herniated because the joint wasn't moving correctly.
And until that joint's corrected, no amount of core strengthening will fix the problem.
That's the mechanical reality. That's the root cause. And that's what individualized, root-cause chiropractic care addresses first — before anything else.
If the core exercises you've been doing aren't working, that's not a mystery. It's a mechanical problem.
A chiropractic assessment at Touch of Wellness Chiropractic starts with identifying the exact spinal segment causing the disc injury. Not a generalized "your back is weak" diagnosis.
A specific evaluation of which joint isn't moving correctly, what's restricting it, and how that's affecting the nervous system's ability to control the stabilizers.
The care plan's built from what you actually report — not from a protocol sheet. If something isn't producing results after a few visits, it changes. Not repeated. Changed.
The willingness to reassess is what separates root-cause care from cookie-cutter care.
Find out what your spinal mechanics assessment reveals.
If your disc injury's been blamed on weak abs, but the exercises haven't fixed it, that's not because you haven't done enough planks. It's because no amount of planks will correct a mechanical fault at the joint level.
Copyright Touch of Wellness Chiropractic 2026
1101 W Jackson St, Suite A Morton, IL 61550
Web Design by iTech Valet